
In the field of In Vitro Fertilization (IVF), uterine fibroids have long stood as a primary clinical variable. Depending on their size and localized anatomical position, specialists carefully weighed the necessity of surgical removal, and myomectomy frequently served as the baseline starting point for a patient’s reproductive strategy.
However, recent landmark data is fundamentally challenging this familiar premise.
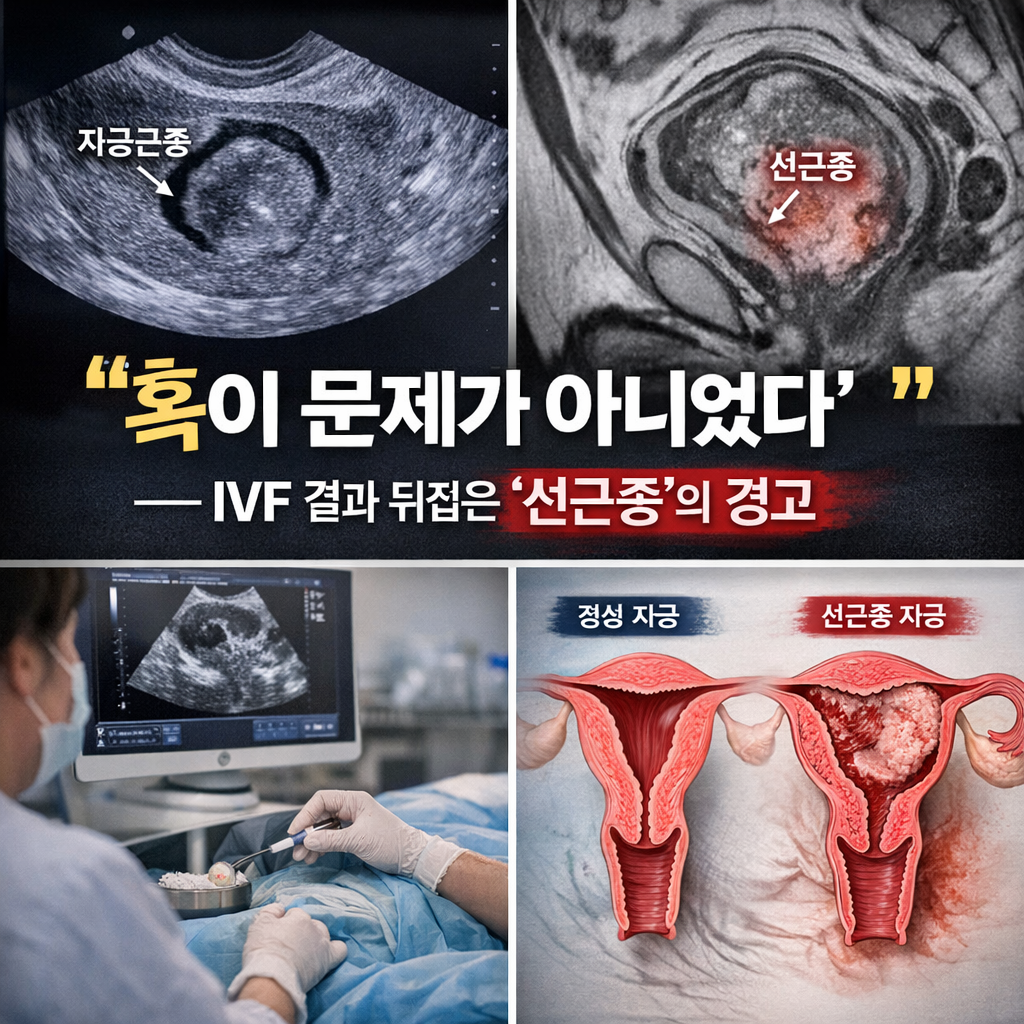
The clinical focus is shifting away from traditional fibroids, steering toward an entirely different uterine pathology.
A comprehensive IVF cohort study evaluating approximately 971 patients highlighted findings that turn conventional clinical assumptions on their head. Statistically, the patient cohort presenting with simple uterine fibroids demonstrated no significant negative variance in overall pregnancy outcomes.
Conversely, the clinical reality for patients diagnosed with adenomyosis (자궁선근증) was starkly different. The second-trimester miscarriage rate within the adenomyosis cohort surged to approximately 35.7%, an overwhelmingly disproportionate figure compared to the 6.4% documented in the healthy control group.
This disparity carries profound clinical implications that extend far beyond raw statistical charts.
A fibroid is essentially an isolated localized tumor. While it occupies physical space and can mechanically impede embryo implantation depending on its location, it remains a structurally demarcated entity that can be surgically resected.
Adenomyosis, however, operations on an entirely different pathological plane. It is a condition where endometrial glandular tissue abnormally infiltrates deep into the surrounding myometrium (uterine muscular layer). In essence, the baseline quality of the uterine tissue itself undergoes a degenerative structural shift. Simply put, the core problem is no longer a localized hazard on the surface; the entire biological soil has become hostile.
In active clinical practice, this pathological distinction dictates everything.
A fibroid is a highly visible, measurable disease. It can be easily mapped via transvaginal ultrasound, its diameter can be precisely tracked, and its eligibility for removal can be clearly defined.
Adenomyosis offers no such clarity. It is a diffuse, ill-defined disease with blurred margins that systematically alters the uterus’s global contractility, micro-vascular blood flow, and localized inflammatory environment. Ultimately, it constructs a hostile intrauterine environment where even if an embryo successfully completes initial implantation, the structural matrix fails to sustain the pregnancy long-term.
Traditional IVF transfer strategies have historically been relatively straightforward: optimize embryo quality in the lab and transfer the blastocyst at the precise endometrial window. The uterus’s capacity to sustain gestation was largely treated as a secondary consideration.
Today, that clinical hierarchy is being inverted. The holistic physiological state of the uterus is emerging as a variable that dictates outcomes just as heavily as—if not more than—intrinsic embryo quality.
Crucially, adenomyosis is not merely a barrier to initial implantation. The most critical takeaway from this recent cohort study addresses the phase following successful conception. The pregnancy is achieved, yet it cannot be biologically maintained.
This specific failure mode imposes a far more devastating psychological and physical burden on the patient. It forces couples to endure a recurring cycle of grief—experiencing a profound loss at the exact moment they believed they had finally neared their ultimate goal.
How, then, must our clinical strategies adapt to this paradigm shift?
The core diagnostic question must steer away from simply asking, “Should we surgically remove this fibroid?” Instead, it must transition to: “Does this comprehensive uterine environment possess the biological capacity to sustain a pregnancy to full term?”
Consequently, systemic interventions targeting the invisible environment—such as down-regulatory hormonal suppression therapies, advanced endometrial priming protocols, targeted anti-inflammatory management, and uterine blood-flow optimization—are rightfully moving to the absolute center of advanced fertility care.
The discipline of reproductive endocrinology is becoming increasingly precise. The paradigm is shifting from a technology focused solely on generating viable embryos to a comprehensive science that meticulously maps out the gestational path long after implantation has concluded. Throughout this evolution, one biological truth remains absolute: a pregnancy may begin with successful fertilization, but it is fulfilled only through sustained gestation.
The message delivered by this research is definitive. We must look past the visible, isolated lesions and focus intensely on the micro-environmental health of the uterus. For decades, fibroids have been clinically overestimated simply because they are highly visible, while adenomyosis has been chronically underestimated because its boundaries remain deeply hidden beneath the surface.
Editor’s Note: This content is an analytical commentary prepared by a specialized medical journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment plans must exclusively be established through direct consultation with a qualified fertility specialist.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.