
A 38-year-old woman (Ms. Lee), married for two years, recently visited a fertility clinic due to difficulties conceiving.
Her ultrasound revealed uterine fibroids—four of them, to be exact. The sizes varied, with the largest measuring 3.5 cm in diameter. Three were intramural fibroids, located within the muscular wall of the uterus, while one was a submucosal fibroid, growing into the uterine cavity (the hollow space inside the uterus). While intramural fibroids can often be managed with a wait-and-see approach, submucosal fibroids can cause infertility or recurrent miscarriages. Therefore, the medical team recommended a hysteroscopic myomectomy to remove it.
Following a successful surgery that required only a one-day hospital stay, Ms. Lee’s symptoms improved significantly. She currently undergoes routine checkups every six months. More importantly, she is now pregnant with her first child and is looking forward to giving birth in just a few months.
Lately, an increasing number of patients find themselves in a similar situation to Ms. Lee. Uterine fibroids, one of the most common gynecological conditions, are benign (non-cancerous) tumors that develop from the abnormal proliferation of smooth muscle cells within the uterine wall. Notably, patients in their 20s and 30s—the primary childbearing years—account for nearly 20% of all cases, with 9,359 and 60,863 patients respectively.
The exact cause of uterine fibroids remains unclear. However, known risk factors include nulliparity (never having given birth), early onset of menstruation, a first pregnancy after age 30, obesity, diabetes, hypertension, and a family history of fibroids. Additionally, dietary factors such as exposure to environmental hormones, alcohol consumption, and caffeine intake are reported to play a role.
Uterine fibroids are frequently asymptomatic. Yet, in about 30% to 40% of cases, patients experience a range of symptoms depending on the location and size of the tumors. The most common signs are menorrhagia (heavy menstrual bleeding) and abnormal uterine bleeding. When severe, this bleeding can lead to iron-deficiency anemia.
Depending on their size and position, fibroids can also cause pelvic pain or severe cramps (dysmenorrhea). Large fibroids often create a sensation of pelvic pressure or bloating. If they press against the colon, bladder, or urinary tract, they can trigger constipation, frequent urination, urinary urgency, or even abnormal kidney function.
For those who conceive with existing fibroids, the tumors usually stay the same size or shrink, though they can occasionally grow or cause pain. They may also be associated with complications such as preterm labor, breech presentation (where the baby’s buttocks or feet point downward instead of the head), and low birth weight. In severe cases, they can lead to miscarriage, making meticulous prenatal care essential.
Nevertheless, the overall pregnancy prognosis for women with fibroids remains highly favorable. Unless a patient has a history of fibroid-related pregnancy complications from a previous birth, routine myomectomy is generally not recommended during pregnancy solely to prevent complications.
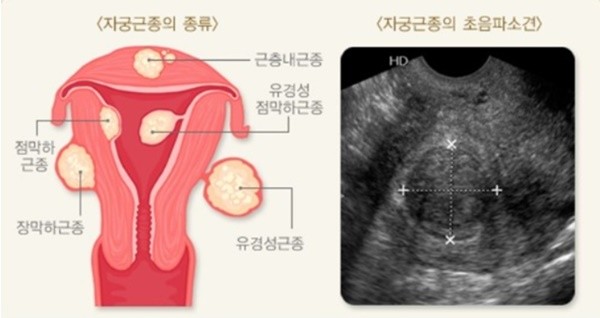
While fibroids come in various sizes upon detection, they are broadly classified into three categories based on their location: subserosal fibroids (protruding outward from the uterus), intramural fibroids (embedded within the muscular uterine wall), and submucosal fibroids (bulging into the uterine cavity).
The treatment protocol for uterine fibroids is highly individualized. It requires a comprehensive evaluation of the tumor’s size and location, the presence of symptoms, the patient’s age, and her future family planning goals. If the fibroids are small and asymptomatic, regular monitoring to track changes in size and symptoms is typically sufficient.
However, women of reproductive age require active and precise management, as the specific location or size of a fibroid can be a direct cause of infertility or recurrent miscarriages. Surgery becomes necessary if, like Ms. Lee, the fibroid resides inside the uterine cavity or distorts its shape. If the fibroid is small and does not impact the uterine cavity, monitoring is completely adequate and pregnancy can proceed smoothly.
Treatment may also be required if symptoms become severe or if a fibroid grows rapidly. While some patients visit a gynecologist due to noticeable symptoms, others discover their fibroids entirely by chance during a routine ultrasound after becoming pregnant.
For unmarried women or those planning a future pregnancy who require intervention, medical (drug) therapy can be considered first alongside regular monitoring. If surgical intervention becomes inevitable, a myomectomy—which removes only the fibroids while preserving the uterus—is performed.
On the other hand, if a patient experiences severe abnormal uterine bleeding, pelvic pain, or rapid fibroid growth and has no future childbearing plans, a hysterectomy (removal of the uterus) may be performed. Of course, non-surgical or minimally invasive alternatives that preserve the uterus are also available, including uterine artery embolization (UAE), High-Intensity Focused Ultrasound (HIFU), and myolysis.
In very rare instances (about 0.1% to 0.3% of cases), uterine sarcoma—a type of cancer—is diagnosed during fibroid surgery. However, patients with asymptomatic fibroids should not undergo a preemptive hysterectomy out of fear that the benign tumor will turn into sarcoma.
For prevention, it is highly recommended that unmarried women and those planning a family undergo regular gynecological screenings, even in the absence of symptoms. If you are diagnosed with uterine fibroids, consulting a reproductive specialist is the best way to design a personalized management and treatment roadmap tailored to your body.

Medical Advisor: Dr. Young Sik Choi, Professor of Obstetrics and Gynecology (Infertility and Reproductive Endocrinology Division) at Severance Hospital.