For those undergoing In Vitro Fertilization (IVF), few phrases are as demoralizing as: “The embryo was perfect, but it didn’t implant.” When you have done everything right—optimized your health, stimulated your ovaries, and nurtured your embryos to blastocyst stage—a failed transfer feels less like a biological outcome and more like a mysterious defeat.
However, reproductive medicine is increasingly recognizing that the uterus is not a restaurant open 24/7. It is more like an appointment-only boutique: it only opens its doors for a brief period known as the “Window of Implantation.”
The Precision of Timing Standard IVF protocols assume that every woman’s window of implantation occurs at the same time: typically five days after the start of progesterone exposure. While this “textbook” timing works for the majority, clinical data suggests that for roughly one in three women, this schedule is out of sync.
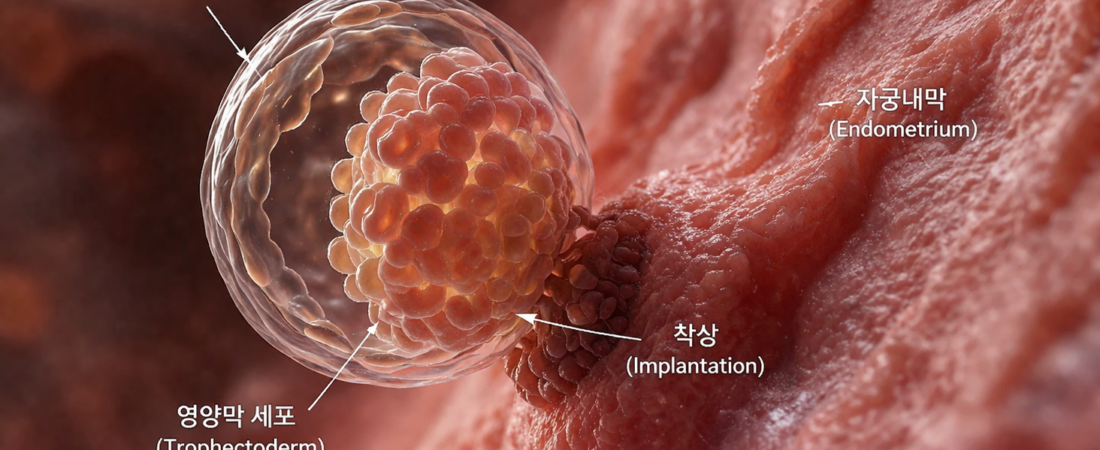
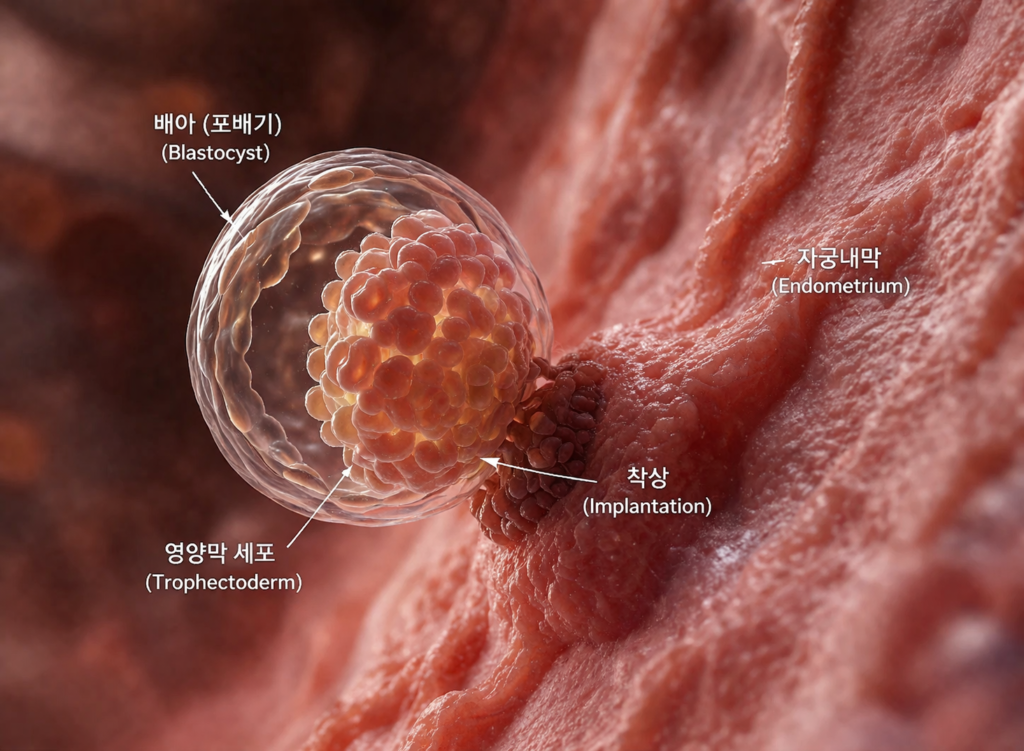
In some patients, the window opens late; in others, it has already closed. If the embryo arrives when the door is locked, implantation cannot occur, regardless of how “perfect” the embryo may be.
Enter the ERA Test: Personalizing the Schedule The Endometrial Receptivity Assay (ERA) was developed to solve this timing mismatch. Rather than guessing based on general averages, the ERA analyzes the expression patterns of over 200 genes within the endometrial tissue. By performing a biopsy at the time when the window is expected to open, clinicians can determine if your specific biological clock matches the standard protocol.
The results are often eye-opening: approximately 30% of patients who undergo the ERA test discover that their optimal window of implantation is different from the standard. For these individuals, every previous transfer was an attempt to enter a building before the doors were unlocked or after they had been bolted shut.
Who Should Consider the ERA? It is important to emphasize that the ERA is not a “cure-all” and is not recommended for every IVF patient. It is a specialized tool, most beneficial for:
- Recurrent Implantation Failure (RIF): Patients who have undergone multiple failed transfers despite using high-quality blastocysts.
- Patients with Unexplained Infertility: Those who have ruled out structural uterine issues, immunological factors, and other common barriers, yet remain unsuccessful.
- Those with High-Quality Embryos: Since the test requires a biopsy of the lining, it is most relevant when a patient has confirmed the ability to produce viable, 5-day blastocysts.
The Goal: Not More Embryos, but Better Synchrony The ERA test does not magically increase the quality of your embryos or the overall pregnancy rate for the general population. Instead, it serves as a “precision diagnostic” for those suffering from a timing mismatch. It turns the IVF process from a “best guess” scenario into a personalized, synchronized event.
Conclusion: Persistence Requires Precision If you are currently facing repeated failures, please understand that your infertility may not be a reflection of a biological inability to conceive, but rather a simple—though heartbreaking—case of poor synchronization.
Medicine is moving away from the “one-size-fits-all” approach. If your embryo transfers continue to result in failure, don’t just blame the embryo or yourself. Ask your fertility specialist about the “window of implantation.” Sometimes, the solution isn’t found in a new stimulant or a stronger dose of medication, but in the patience and precision of finding your own, unique biological schedule.
Sources: Clinical literature on Endometrial Receptivity Assay (ERA); research on gene expression in the endometrium; reproductive medicine guidelines on recurrent implantation failure.
Disclaimer: This report is for informational purposes. The ERA test is a specialized diagnostic procedure; discuss its necessity with your reproductive endocrinologist based on your specific treatment history.