When assessing ovarian function, we look at a constellation of factors. While ovarian volume (via ultrasound) and basic blood markers like FSH (Follicle-Stimulating Hormone) and Estradiol (E2) provide a snapshot of current hormonal responsiveness, one metric stands out for its reliability: AMH (Anti-Müllerian Hormone).
What Does AMH Really Tell Us? AMH is secreted by the small, pre-antral follicles (2–6mm) within the ovaries. Because it originates directly from these follicles, it serves as a proxy for the total “reserve” of follicles left—the pool of potential eggs available for the future. Unlike FSH, which fluctuates significantly throughout a cycle, AMH remains relatively stable, making it the most consistent indicator of ovarian reserve.
Interpreting the Numbers Clinically, AMH is often used as a rough guide to “ovarian age.” While these benchmarks vary by laboratory, they provide a general framework:
- AMH ~4.0 ng/mL: Corresponds roughly to the late 20s.
- AMH ~3.0 ng/mL: Corresponds roughly to the mid-30s.
- AMH ~2.0 ng/mL: Corresponds roughly to the late 30s.
- AMH ~1.0 ng/mL: Often reflects the early 40s.
- AMH < 0.5 ng/mL: Indicates a significantly diminished reserve, often associated with a shorter window before menopause.
Conversely, values above 8.0 ng/mL often prompt an investigation for Polycystic Ovary Syndrome (PCOS).
The Important Distinction: Quantity vs. Quality The most critical takeaway for patients is this: AMH reflects the quantity of your ovarian reserve, not the quality of the eggs.
A higher AMH does not automatically guarantee higher quality or a higher chance of a genetically normal embryo, especially as maternal age advances. Even with a decent reserve, age remains the dominant factor determining the chromosomal health and viability of the eggs. Therefore, AMH should never be viewed as a standalone measure of pregnancy potential; it must be interpreted alongside your chronological age, chromosomal health, and overall reproductive environment.
The Speed of the Ovarian Clock Furthermore, AMH helps us estimate the “velocity” of ovarian decline. Statistical modeling suggests that for a patient with an AMH of 0.1 ng/mL, the timeline to menopause might be only a few years, whereas the same value in a younger patient might represent a longer duration of remaining fertility. Ovarian function does not necessarily decline linearly; it often accelerates as a woman approaches menopause.
Conclusion: A Compass, Not a Verdict In modern fertility care, we rely on three pillars to assess your ovarian status:
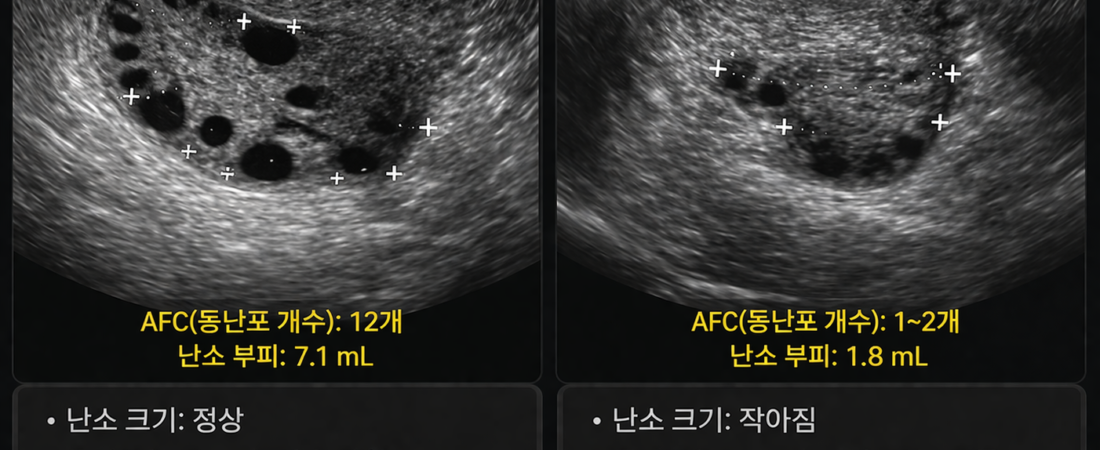
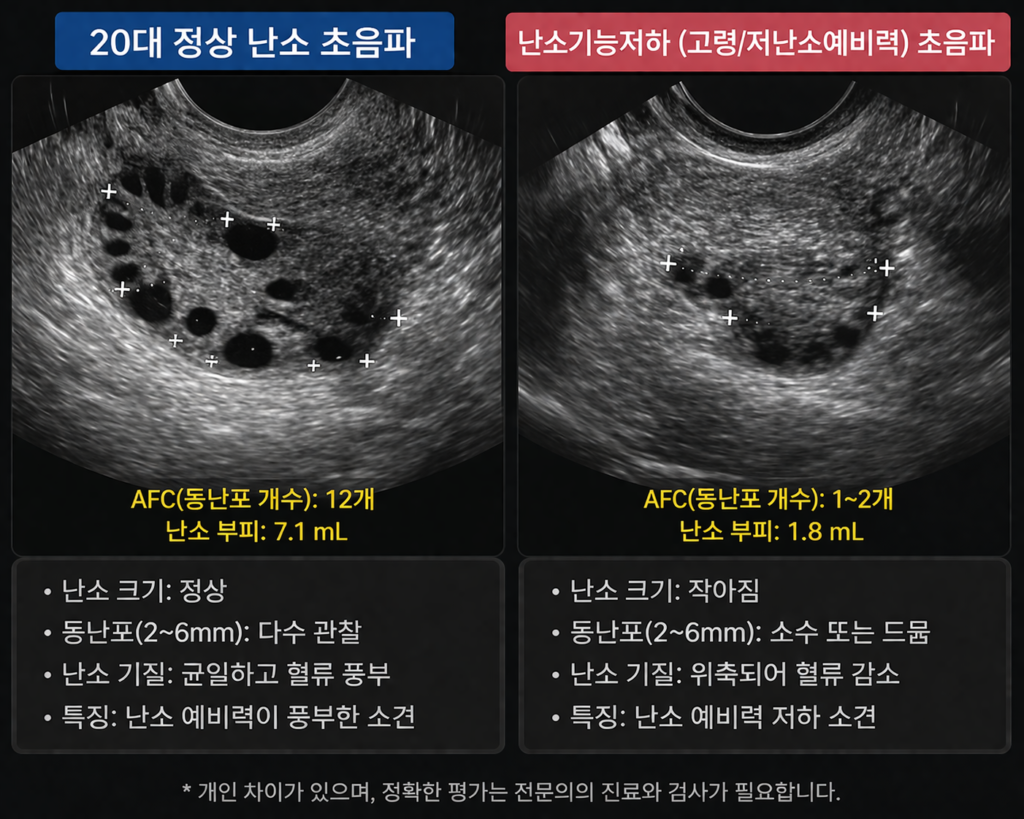
- Ultrasound: To assess structural health and antral follicle count (AFC).
- Hormonal Markers (FSH/E2): To measure current responsiveness.
- AMH: To gauge the remaining reserve.
Do not allow your AMH number to define your identity or dictate your future. It is not a verdict on your reproductive potential, but a compass that tells us how fast the ovarian clock is ticking. By understanding where you stand today, you can make informed, proactive decisions about your family-building strategy.
Sources: Clinical guidelines on Ovarian Reserve Testing; longitudinal data on AMH levels and reproductive aging; international reproductive endocrinology consensus.
Disclaimer: This report is for informational purposes. Ovarian reserve testing is complex; always review your specific AMH results and their clinical implications with a board-certified reproductive endocrinologist.