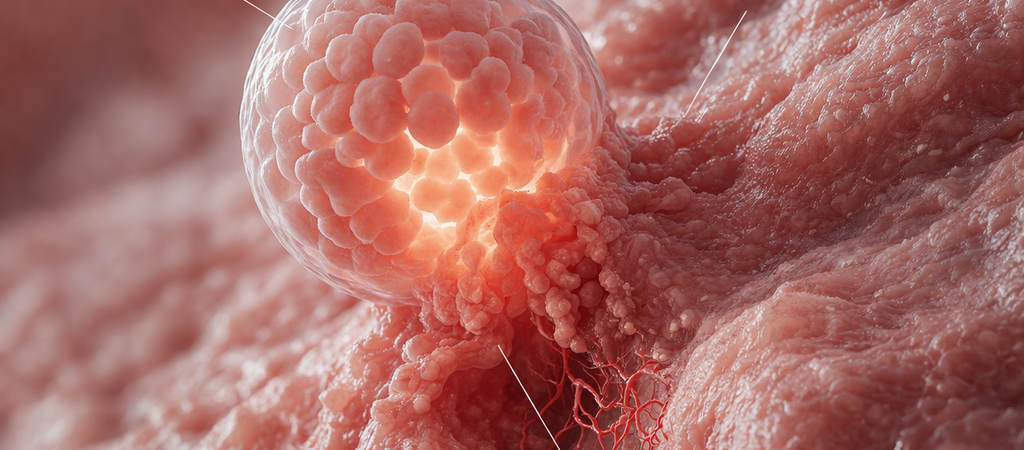
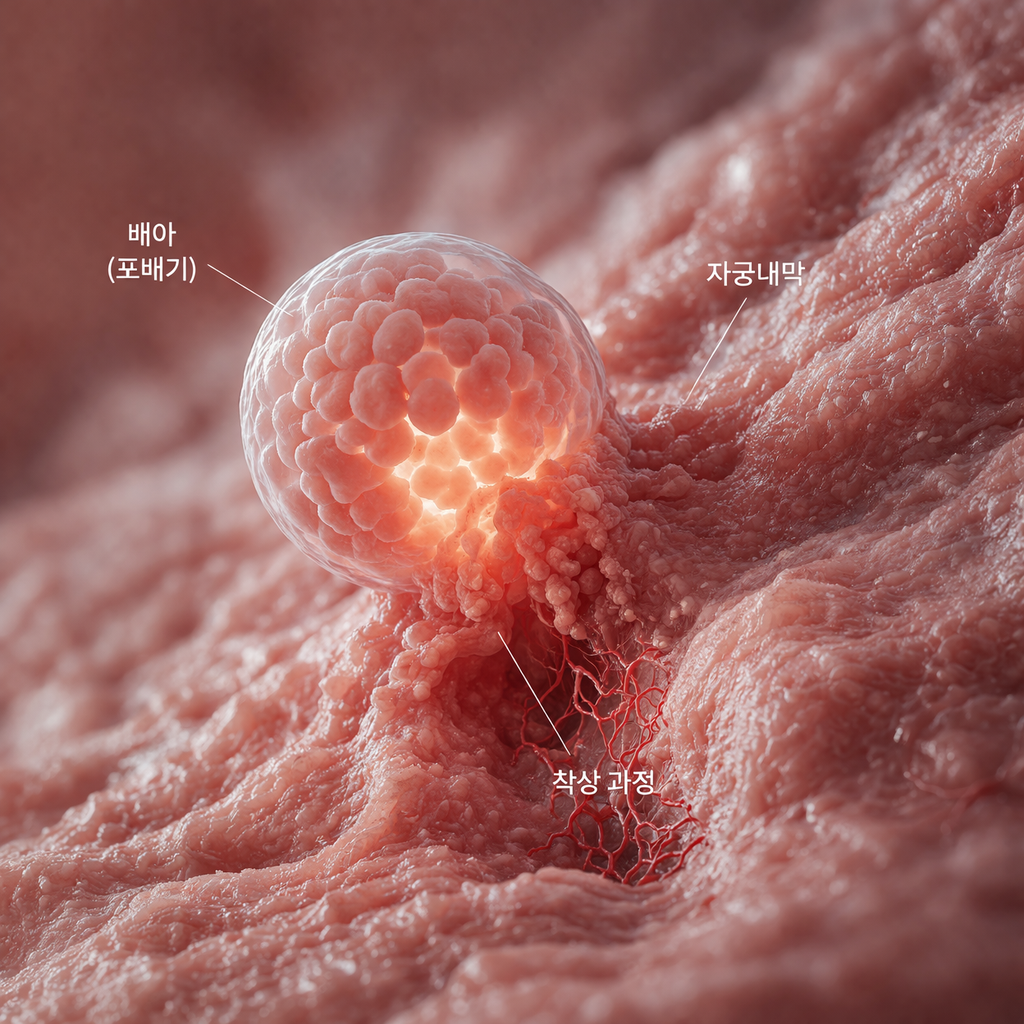
Achieving a successful implantation is the definitive beginning of pregnancy.
The endometrium (자궁내막) is not a static structure; it is a highly dynamic, living tissue responsible for allowing the embryo to attach, invade, and establish vital vascular connections. This complex biological milestone is what we define as implantation (착상).
When patients navigating infertility are informed by their clinician that their endometrial lining is thin, they almost universally fixate on a flat numerical value—7 mm, 8 mm. There is a deep, widespread belief that failing to surpass this standardized baseline renders conception impossible. This clinical understanding, however, is only half-taught. In fact, within the active landscape of reproductive endocrinology, it is occasionally entirely inaccurate.
In clinical reality, scenarios where a patient repeatedly experiences cycle failures despite possessing an endometrial thickness exceeding 8 mm are remarkably common. Conversely, successful full-term pregnancies achieved within the 6 mm range are undeniably documented. At this precise juncture, the core diagnostic question must be fundamentally reframed:
Is the raw thickness of the endometrium truly the primary barrier?
The uterine lining is not a lifeless brick wall. It is an intricate, highly coordinated functional system engineered to biochemically receive and integrate a developing embryo. It is a multi-factorial organ that modulates synchronized blood flow, responds dynamically to systemic steroid hormones, and actively regulates localized immunological responses. The exact moment this internal system fractures, raw thickness loses all clinical significance. A thin endometrium is never an isolated primary cause; it is a downstream consequence—a signal indicating that the underlying biological machinery has already been compromised.
Consequently, the initial phase of clinical intervention traditionally centers around hormonal manipulation.
Clinicians systematically attempt to drive endometrial proliferation by supplementing exogenous estrogen. Patients ingest oral tablets, apply transdermal patches, and utilize vaginal inserts. While this baseline protocol is common knowledge, real-world application reveals that certain women exhibit an absolute non-responsiveness to these hormones, regardless of the dosage.
Yet, the exact millisecond the clinical team alters the route of administration, the dormant endometrium can suddenly undergo a robust proliferation. This radical divergence is dictated not by raw pharmacological volume, but by the precision of the delivery mechanism. The endometrium is an extraordinarily hyper-sensitive tissue; it cannot be forced to grow through simple over-supplementation.
Following hormones, the next critical variable is vascular perfusion (혈류 흐름). This factor resides far closer to the biological core of the pathology. The endometrium is, by its very nature, a dense matrix of micro-vessels. In the absence of robust blood flow, cellular proliferation is physically impossible. To address this micro-vascular deficit, contemporary clinical strategies occasionally deploy intravaginal sildenafil (비아그라) or utilize rheological agents like pentoxifylline to actively optimize micro-circulation. These protocols are frequently paired with low-dose aspirin.
The clinical outcomes of this approach are highly compelling: the exact moment the micro-vascular networks are opened, an endometrial lining that remained completely stagnant for months can suddenly exhibit a sharp physiological response. This clear pattern demonstrates that the underlying pathology was never a question of raw thickness, but rather a discipline of vascular supply.
In cases where the endometrium remains completely refractory—demonstrating zero responsiveness despite aggressive hormonal optimization and targeted vascular therapies—the clinical approach must pivot. The strategy shifts from attempts at forced growth to a philosophy of tissue regeneration. This is the precise arena where advanced therapies like Platelet-Rich Plasma (PRP) enter the reproductive landscape. While it is premature to classify these interventions as the universal standard of care, peer-reviewed literature continuously reports instances where an otherwise completely non-responsive, deadened lining exhibits regular cellular proliferation following regenerative therapy. Ultimately, the diagnostic calculus distills into a single question: Is this specific endometrium in a state capable of growth, or is it in a state requiring complete regeneration?
When dissecting endometrial pathologies, one non-negotiable historical variable must be evaluated.
A medical history featuring historical dilation and curettage (D&C, 소파수술), recurrent intrauterine interventions, or chronic pelvic infections means the lining is not merely thin; it is structurally scarred and damaged. Under these compromised parameters, aggressively elevating systemic estrogen levels is clinically futile. The primary clinical priority must be the mechanical resolution of intrauterine adhesions via operative hysteroscopy (자궁경) or the utilization of localized endometrial scratching. Biological tissue requires a calibrated healing cascade to rebuild itself following trauma. If a clinical team fails to respect this baseline principle, the treatment strategy will continuously miss the target.
What, then, are the underlying root causes driving persistent endometrial thinning?
Chronic endometritis (만성 자궁내막염), intrauterine synechiae (유착), and prolonged endocrine suppression states represent the definitive triad that halts regular endometrial growth. The core clinical challenge is that these specific conditions are notoriously invisible under standard transvaginal ultrasound evaluations. The diagnostic report simply concludes that the lining is “thin.” Driven by this incomplete data, the cycle of failure repeats: the clinician escalates the estrogen dose, the cycle fails, and the dose is scaled up again. Yet, if the underlying soil has been completely degraded, pouring infinite amounts of water onto the surface will yield zero absorption.
Therefore, an advanced fertility protocol evaluates vascular perfusion first, verifies real-time endocrine responsiveness second, checks global structural architecture third, and analyzes raw thickness last.
Countless patients remain intensely obsessed with the standardized 7 mm baseline threshold. However, this numerical marker must be treated strictly as a generalized reference value. The definitive clinical variable is whether the endometrium resides in an actively receptive, open state. The ultimate focus is whether the lining possesses the exact molecular readiness required to capture and sustain an incoming embryo the moment it enters the uterine cavity. We must never forget that regardless of how biologically perfect an embryo may be, a successful pregnancy can only initiate when implantation is fully realized.
📚 Medical References
- European Society of Human Reproduction and Embryology (ESHRE)
- Clinical Practice Guidelines on Endometrial Receptivity and Implantation.
- Significance: The definitive global consensus framework detailing the molecular, immunological, and structural criteria that govern successful blastocyst attachment.
- American Society for Reproductive Medicine (ASRM)
- ASRM Practice Committee Reports on Endometrial Thickness and Assisted Reproductive Outcomes.
- Significance: Extensive epidemiological evaluations demonstrating the statistical variance, success boundaries, and clinical limitations of utilizing raw endometrial thickness as an isolated predictor of live birth rates.
- Fertility and Sterility & Human Reproduction
- Selected Cohort Studies on Endometrial Receptivity, Vascular Perfusion, and Implantation Kinetics.
- Significance: Peer-reviewed clinical trials demonstrating that micro-vascular blood flow indices and endometrial wave patterns dictate implantation competency far more reliably than simple millimeter measurements.
- Reproductive Biology and Endocrinology
- Mechanistic reviews on uterine micro-circulation and sildenafil/pentoxifylline therapies.
- Significance: Outlines the specific pharmacological pathways used to reverse localized ischemic states within refractory endometrial tissues.
- Journal of Assisted Reproduction and Genetics
- Clinical evaluations of autologous Platelet-Rich Plasma (PRP) in refractory thin endometrium.
- Significance: Landmark regenerative medicine research documenting the statistically significant upregulation of tissue proliferation markers following targeted intrauterine PRP infusions.
Editor’s Note: This content is an analytical commentary prepared by a specialized fertility journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment decisions must exclusively be established through direct consultation with a qualified medical professional.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.