Worth a Try for Repeated Implantation Failure, Despite the High Cost—But Only with Blastocyst-Stage Embryos
Among women navigating the challenges of infertility, Endometrial Receptivity Analysis (ERA) has recently become a hot topic. Introduced to South Korea in 2018, the ERA test was developed by IGENOMIX in Spain through a decade of clinical research. In simple terms, it is a diagnostic tool designed to find the optimal biological window for the uterus to receive an embryo.
“Endometrial receptivity” refers to a specific state in which the endometrium becomes permissive to a blastocyst (a day-5 embryo). An embryo attempts to implant during the late blastocyst stage—around the time it finishes hatching, sheds its zona pellucida, and transitions from a “snowman” shape to an expanded “potato” shape.
However, a successful implantation requires more than just the embryo’s effort. The endometrium must also be fully prepared to welcome it. This specific timeframe is known as the “implantation window.” The endometrium opens this window a certain number of days after ovulation, and timing is absolutely everything; the embryo and the uterine lining must be perfectly synchronized for implantation to succeed.
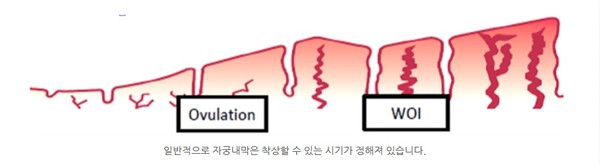
During In Vitro Fertilization (IVF), embryos cultured outside the body are transferred back into the uterus. This transfer must occur precisely when the endometrium has opened its implantation window wide. Textbooks state that based on a standard 28-day menstrual cycle with ovulation on day 14, this window opens around day 18 and closes around days 21 to 22. However, the human body is not programmed to be exactly the same every single month.
To put it simply, once ovulation occurs and progesterone is secreted, the implantation window opens roughly five days later. Consequently, during a frozen embryo transfer (FET) cycle, a day-5 blastocyst is transferred exactly five days after the patient is first exposed to progesterone.
Yet, this textbook schedule does not apply universally to every woman. If a patient’s unique endometrial environment deviates from this standard timeline, performing an FET strictly by the textbook can lead to failure. Even with a high-quality embryo, transferring it outside the endometrium’s optimal receptive phase will ultimately prevent implantation.
Does the ERA test actually work? Does it improve implantation rates?
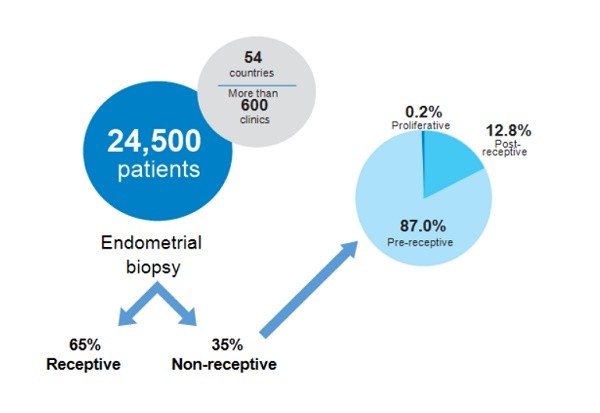
Global data across 54 countries involving approximately 24,500 women revealed that about 35% of them had a non-standard implantation window. Among this group, roughly 87% had a delayed window (shifted by 0.5 to 1 day), while about 13% had an advanced window. In other words, the implantation window opens and closes at different times for different individuals.
Furthermore, according to data presented by ESHRE (European Society of Human Reproduction and Embryology) and ASRM (American Society for Reproductive Medicine), when more than 35,000 patients experiencing recurrent implantation failure (RIF) underwent the ERA test, over 25% were found to have a standard transfer date that was completely unsuited for implantation.
Given this significant correlation between ERA results, personalized frozen embryo transfers, and subsequent pregnancy rates, how exactly is the test performed?
First, an ERA test cannot be conducted during an ovarian stimulation cycle. It must be carried out during a dedicated frozen embryo transfer cycle, and the insights gained are then applied to the subsequent actual transfer cycle.
To obtain an endometrial tissue sample, the preparation mimics a real FET cycle precisely. Starting from day 2 or 3 of the menstrual cycle, oral estrogen (such as Progynova) is administered to thicken the uterine lining. Progesterone is then introduced, and exactly five days later—the typical timing for an embryo transfer—an endometrial biopsy is performed to collect a tissue sample.
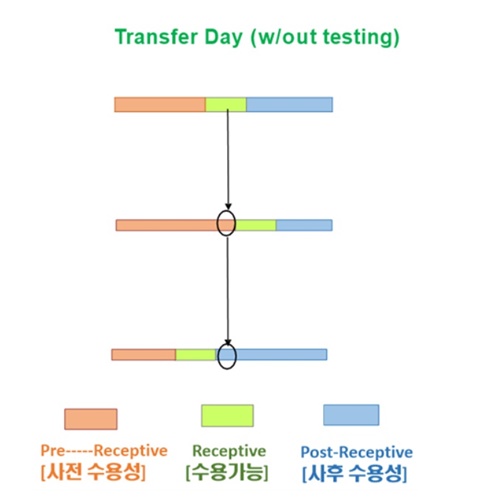
The collected tissue is sent to Spain, where the expression levels of 236 RNA genes are rigorously analyzed. This analysis reveals whether the endometrium on the fifth day of progesterone exposure was “Receptive” (Phase A), “Pre-receptive” (Phase B), or “Post-receptive” (Phase C).
These results dictate the timing of the next actual frozen embryo transfer. For a “Pre-receptive” result, the day-5 blastocyst will be transferred more than five days after starting progesterone. Conversely, for a “Post-receptive” result, the transfer will be scheduled earlier than the standard five-day mark.
Hearing this, you might wonder, “Should I get this test done to boost my chances?” Not necessarily.
The ERA test is not recommended for everyone across the board. Specialists typically advise it only when a patient has experienced multiple unexplained implantation failures despite a healthy uterine lining and high-quality embryos, or when standard repeated implantation failure screenings reveal absolutely no underlying issues.
Crucially, patients must be able to produce day-5 blastocysts to safely consider this route. It is highly recommended for those who face total implantation failure across multiple IVF cycles without a clear cause, or for older patients (in their 40s) who have experienced frequent implantation failures.
The ERA test is actively utilized in fertility clinics. In one notable evaluation of 50 patients who had failed more than five standard cycles without a clear cause, 30 women successfully achieved pregnancy after adjusting their frozen embryo transfer timing based on their ERA results.
Ultimately, pregnancy hinges on successful intrauterine implantation. While an embryo must clear several biological hurdles to implant, the success of the process depends primarily on the endometrial environment and embryo quality. Given that a decrease in endometrial receptivity accounts for roughly 60% of all implantation failures, this test is well worth considering for those facing repeated, unexplained setbacks—even with its high price tag.
The world of implantation is undeniably complex. Consider it like this: to enjoy a specific dish at a train station, you must arrive precisely at the scheduled hour. Arriving too early or too late means missing the opportunity entirely. Furthermore, to be served, the environment must be in its perfect “receptive” state.
Ultimately, just as an embryo has a specific time it must implant, the endometrium has a precise window to receive it. Even a top-tier embryo will fail if that fleeting, crucial window of synchronization is missed.
Beyond timing, a completed implantation requires the embryo to divide without chromosomal abnormalities, adequate levels of hCG and progesterone, a lack of maternal immune rejection, and most importantly, a plush, adequately thickened uterine wall ready for the embryo to burrow into. Only when all these elements align can the embryo securely implant and begin its full development.
Medical Advisor: Dr. Kyung Yong Moon, Medical Director at iORA Fertility Clinic.