If you have been diagnosed with a hydrosalpinx (난관수종) in your fallopian tubes, is it clinically wiser to completely resolve it via surgical removal (salpingectomy), or is it better to opt for a non-surgical intervention?
To answer this, let us first explore what causes a hydrosalpinx.
Within the female reproductive tract, the fallopian tubes play an indispensable role in natural conception. They serve as the literal site of fertilization where the egg and sperm meet. Consequently, if a fallopian tube becomes blocked, natural pregnancy becomes highly unlikely, and even Intrauterine Insemination (IUI) yields minimal success.
Why exactly does a hydrosalpinx form? When the distal end of a fallopian tube becomes occluded (blocked), normal mucosal secretions and cellular fluids become trapped inside, causing the tube to distend into a fluid-filled sac. Under normal physiological conditions, fallopian tube fluid drains naturally into the pelvic cavity. However, when a blockage occurs, this accumulated, often toxic fluid can flow backward into the uterine cavity.
In this state, natural conception is severely hindered because egg and sperm cannot physically meet. Furthermore, even if a couple proceeds with In Vitro Fertilization (IVF), the backward leakage of this hydrosalpinx fluid into the uterus compromises the endometrial environment. When a high-quality embryo cultured in the lab is transferred, this toxic fluid can wash through the uterine cavity, destabilizing the endometrium and actively preventing the embryo from successfully implanting.
Choosing the Right Path: Surgical Removal vs. Non-Surgical Management
When it comes to treating a hydrosalpinx in patients seeking pregnancy, medical philosophies among fertility specialists vary. Some pro-surgery specialists advocate for a clean slate via laparoscopic salpingectomy (난관 절제술), while pro-conservative specialists prefer preserving the anatomy through non-surgical interventions.
There is no single correct answer; it is entirely dependent on the specific clinical case. A clinician must carefully weigh variables such as the severity of the hydrosalpinx, the patient’s baseline ovarian reserve, and the overall state of the uterus.
Fertility specialists who lean toward surgical removal argue:
“Because the fluid within a hydrosalpinx directly impairs embryo development and endometrial receptivity, performing a salpingectomy to remove the blocked tube prior to an IVF embryo transfer significantly boosts pregnancy success rates and increases the likelihood of a healthy live birth.”
From their clinical perspective, unless the underlying implantation environment is fundamentally corrected, achieving a pregnancy remains an uphill battle. However, they also note that unless the hydrosalpinx is exceptionally severe or highly visible on an ultrasound, patients may attempt initial conception cycles before jumping straight to the operating room.
Conversely, with the modern demographic shift toward advanced maternal age and a corresponding rise in patients dealing with diminished ovarian reserve (DOR), an increasing number of women are actively opting for non-surgical interventions. The most prominent among these is ultrasound-guided sclerotherapy (알코올 경화술), a technique used to drain and ablate the fluid sac. This preference is driven by a serious clinical concern: the potential for surgical removal to inadvertently accelerate ovarian depletion.
The anatomical rationale is clear: when surgically removing a fallopian tube to clear a hydrosalpinx, there is an inherent risk of compromising the utero-ovarian vascular network. If the ovarian arteries undergo collateral damage, the blood flow delivering essential oxygen and nutrients to the ovary can drop. Furthermore, if the fallopian tube is severely adhered (attached) to the ovary, the delicate process of peeling them apart can mechanically damage clusters of microscopic primordial follicles, causing a sharp, irreversible drop in the patient’s remaining egg count.
For women already battling low ovarian reserve, non-surgical sclerotherapy is often strongly recommended. Advocates argue that even in severe cases of hydrosalpinx, blindly rushing into a salpingectomy should be avoided, as non-surgical management is vastly superior for conserving precious ovarian tissue.
How Hydrosalpinx Sclerotherapy Works
The mechanism behind ultrasound-guided sclerotherapy is straightforward. Utilizing a specialized needle identical to the one used during an IVF egg retrieval, the clinician aspirates (drains) the trapped fluid from the fallopian tube. The empty cavity is then thoroughly rinsed with a saline solution followed by a concentrated medical alcohol (ethanol) solution to ablate the internal lining and prevent fluid from reaccumulating.
While this is considered a more conservative approach compared to total surgical removal, its primary advantage is that it drastically reduces the physical volume of the hydrosalpinx. This effectively halts the toxic backflow of fluid into the uterus, thereby optimizing the implantation soil.
Consequently, even among fertility patients who do not suffer from diminished ovarian reserve, this non-surgical, outpatient procedure has become highly popular—particularly for working professionals. It requires zero hospitalization, takes a mere 30 to 40 minutes per session, and typically achieves the desired clinical outcome in just two to three brief appointments.
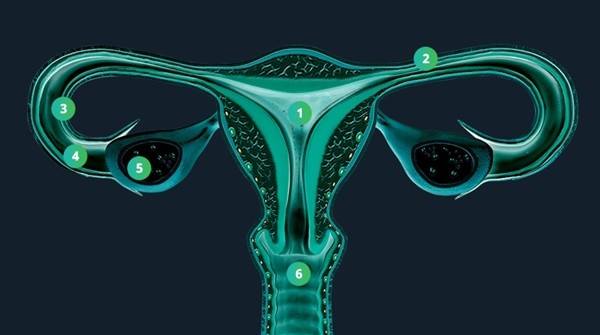
Image courtesy of Maria Fertility Hospital