
“Please do a hysteroscopy first”… The Most Misunderstood Test by Women with Infertility
One of the questions most frequently heard in infertility clinics is about hysteroscopy. In online infertility communities, it is not difficult to come across testimonials like, “I got pregnant right after a hysteroscopy,” “I found the cause of my implantation failure,” or “You must do it before IVF.” There are many women who trust the chatter on internet forums more than their doctor’s advice.
As a result, quite a few women want to undergo a hysteroscopy first, even without a specific medical reason. However, to get straight to the point, a hysteroscopy is not a basic, routine test performed on all women experiencing infertility.
First of all, a transvaginal ultrasound and a hysteroscopy are completely different tests.
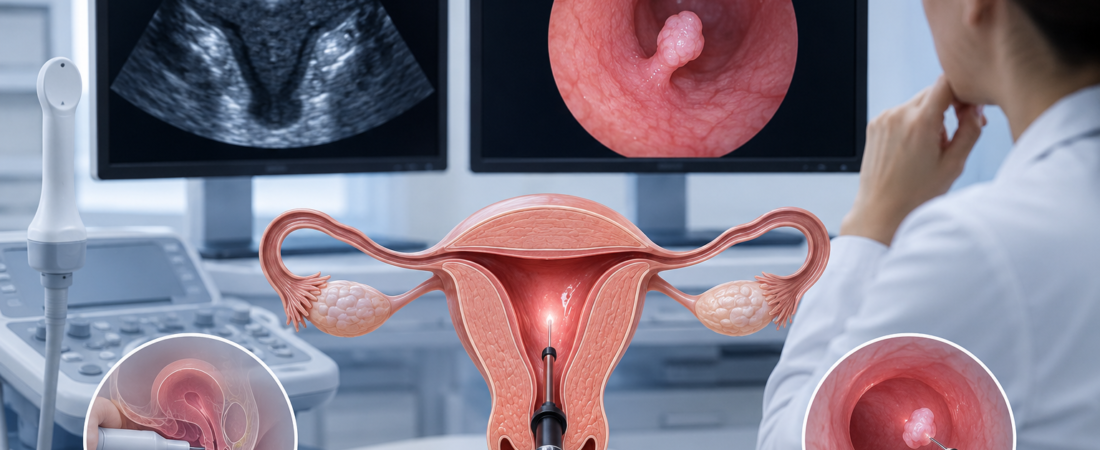
A transvaginal ultrasound involves inserting an ultrasound probe into the vagina and transmitting ultrasound waves from outside the uterus to create an image of the inside. On the other hand, a hysteroscopy is a test in which a thin endoscopic camera, about 3 to 5 mm thick, is inserted directly into the uterus to visually inspect the interior of the uterine cavity.
To put it simply, an ultrasound is like looking inside a house from outside the window, while a hysteroscopy is akin to actually walking into the house to look around.
During a hysteroscopy, saline solution is injected into the uterus to expand the uterine cavity for observation. As the normally touching layers of the endometrium separate, lesions such as small polyps, adhesions, or submucosal fibroids are revealed much more clearly.
Conversely, because a transvaginal ultrasound observes the endometrium while the layers are pressed together against each other, it can sometimes be difficult to distinguish small polyps or lesions lying flat against the uterine wall from the normal endometrial structure.
This does not mean that an ultrasound is an inadequate test. Like myself, doctors who have treated infertility for a long time examine dozens of ultrasounds every day. When tens of thousands of cases of experience accumulate over the years, there are many times when just looking at the screen gives a strong intuition that “there might be a polyp” or “something looks off.” Of course, it is not a definitive diagnosis, but the reasonable suspicion of an experienced doctor often has a remarkably high accuracy rate.
In reality, a significant portion of patients who undergo hysteroscopy are those who already had suspected polyps or uterine cavity abnormalities on their ultrasound. Therefore, one of the reasons there are so many stories of getting pregnant after a hysteroscopy is that the implantation environment improved because polyps or adhesions were removed in a patient group that already had underlying uterine issues. In other words, rather than the hysteroscopy itself magically increasing the pregnancy rate for all women, the results reflect the effect of removing pre-existing lesions.
There is another important fact here: there are certainly cases where no abnormalities were seen on the ultrasound, but lesions are discovered upon performing a hysteroscopy. In actual clinical practice, it is not uncommon to find small polyps, microscopic adhesions, or localized endometrial abnormalities after a hysteroscopy in patients whose ultrasounds appeared perfectly normal.
Particularly among patients who have failed to implant despite transferring good-quality embryos multiple times, unexpected lesions are frequently found. This is exactly why hysteroscopy exists. Ultrasound is an excellent screening test, but it is not perfect, and hysteroscopy can be seen as the ultimate diagnostic tool to check the blind spots that ultrasound might miss.
Then, should every woman with infertility undergo a hysteroscopy? Research results to date say no.
A large-scale randomized trial published in the world-renowned medical journal The Lancet in 2016 showed that performing a routine hysteroscopy before IVF on women with normal uterine cavities on ultrasound did not significantly improve pregnancy and live birth rates.
Since then, major guidelines, including those from the European Society of Human Reproduction and Embryology (ESHRE), have maintained a similar stance. If there are no specific abnormal findings on an ultrasound and no history of recurrent implantation failure or recurrent miscarriage, there is no need to uniformly perform a hysteroscopy on all women with infertility.
Conversely, there are cases where a hysteroscopy should be actively considered.
These include cases with recurrent implantation failure, a history of recurrent miscarriage, suspected polyps or submucosal fibroids on ultrasound, a history of previous uterine surgery, or a possibility of uterine adhesions. In such cases, a hysteroscopy is not just a simple test but a crucial process of finding the root cause blocking the pregnancy.
Above all, the greatest advantage of a hysteroscopy is that diagnosis and treatment can be done simultaneously.
If a polyp is found while observing the inside of the uterus, it can be removed immediately; if adhesions are found, they can be separated. Therefore, a hysteroscopy is closer to a minor surgical procedure than a simple diagnostic test. In fact, many hospitals perform it under twilight anesthesia (sedation), and it is most accurate to understand it as an endoscopy that directly looks inside the uterus, much like a gastroscopy or colonoscopy.
Anyone undergoing fertility treatment becomes anxious. Thoughts arise like, “Is there a test I missed?” or “Wouldn’t doing just one more test increase my chances of getting pregnant?” As a result, certain tests sometimes spread like a fad. However, infertility treatment is not a process of following trends. Medicine must stand on evidence, not on anxiety.
Hysteroscopy is not a necessary test for everyone. However, for patients who truly need it, it can be a decisive intervention that provides the missing clue to pregnancy. It is neither a test to be recommended unconditionally nor a test to be avoided unconditionally. What matters is not the number of tests you take. It is understanding why that specific test is necessary for you right now. Hysteroscopy is no exception to that rule.

Dr. Baek Eun-chan (65), Director of Bundang Cheil Hospital, is considered one of Korea’s leading fertility specialists, having performed over 30,000 IVF procedures. Based on his specialized clinical experience in mild stimulation protocols and recurrent miscarriage treatment, he has focused on treating advanced maternal age infertility and recurrent implantation failure, striving to improve pregnancy success rates through customized fertility treatment strategies.