Many women assume that the uterus is a uniform organ, shaped identically in every woman. In reality, the uterus is a product of complex embryonic fusion—a process where two ducts (the Müllerian ducts) must perfectly merge. Variations in this fusion lead to “uterine anomalies,” a spectrum of shapes ranging from heart-shaped to partitioned or even duplicate structures.
For many, the discovery of a uterine anomaly happens entirely by accident, often during an unrelated medical exam. Because these conditions are congenital and often asymptomatic, many women lead perfectly normal reproductive lives without ever knowing their uterine structure deviates from the textbook norm.
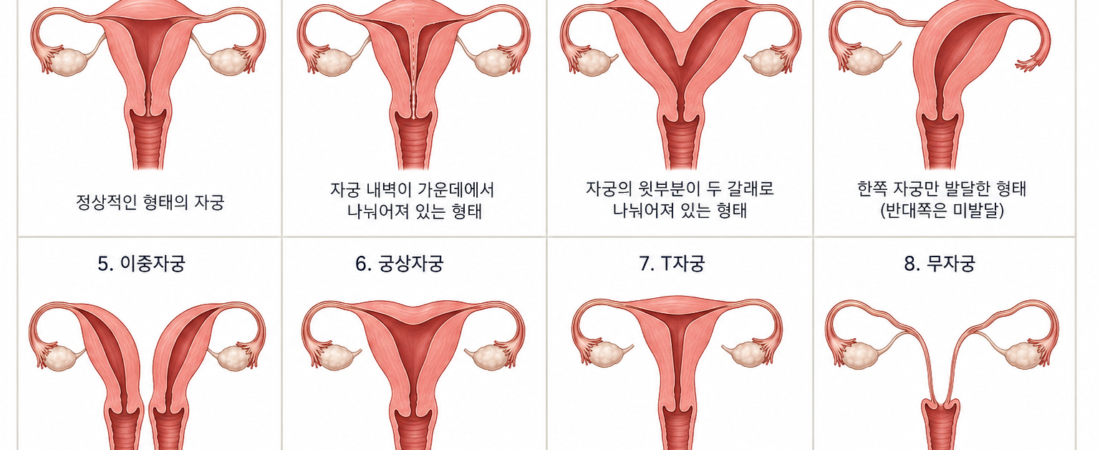
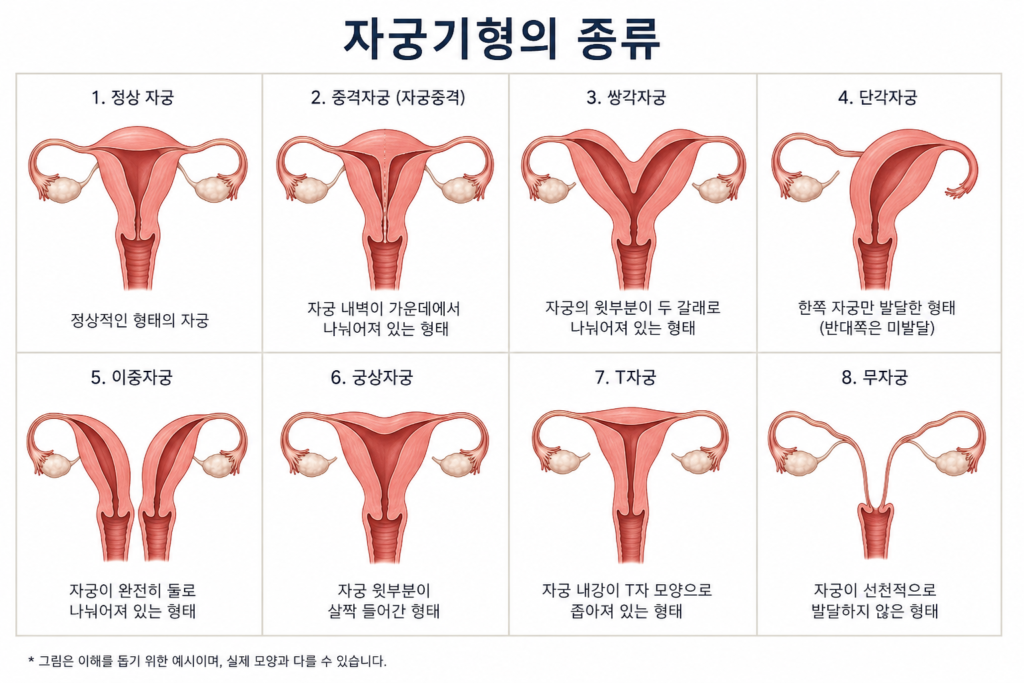
A Spectrum of Anatomy Uterine anomalies are not one-size-fits-all. The clinical implications vary significantly depending on the shape:
- Septate Uterus: A wall (septum) divides the uterine cavity. While it may not look abnormal from the outside, the septum can have poor blood supply, potentially interfering with implantation. It is frequently associated with recurrent pregnancy loss, but often correctable via minor surgery.
- Bicornuate Uterus: The top of the uterus is split, creating a heart-shaped appearance. While this can increase the risk of preterm birth or fetal malposition, many women with this condition conceive and deliver healthy babies without issue.
- Unicornuate Uterus: Only one side of the uterus develops. Because the space is limited, there is a higher risk of preterm birth or fetal growth restriction.
- Didelphys Uterus (Double Uterus): The uterus is fully duplicated. Though it sounds profound, many women with this condition experience normal, successful pregnancies.
- Arcuate Uterus: The top of the uterus is slightly indented. This is so common that many clinicians now consider it a “normal variation” rather than a clinical anomaly, as it rarely impacts fertility.
The Golden Rule: Anatomy is Not Fate The most critical takeaway is this: Anatomical shape does not dictate fertility potential. Internet searches often present uterine anomalies as a barrier to pregnancy, but clinical reality is far more nuanced. We frequently encounter women with significant structural anomalies who conceive naturally and deliver healthy children, while others with minor variations may experience recurrent miscarriage.
Strategic Evaluation If you suspect or have been diagnosed with a uterine anomaly, do not succumb to “search engine anxiety.” The modern diagnostic approach is precise:
- Comprehensive Imaging: 3D ultrasound, HSG (Hysterosalpingography), and MRI allow clinicians to map the uterus with high accuracy.
- Clinical Context: It is essential to remember that uterine development is linked to kidney development during the fetal stage. Specialists often check the kidneys as a precautionary measure, not because the uterus itself is “broken.”
- Personalized Assessment: Treatment is only necessary if the shape is proven to interfere with implantation or pregnancy maintenance. For many, no intervention is needed at all.
Conclusion: Focus on Function, Not Form The medical community has moved away from labeling these variations as “deformities” and toward understanding them as variations in anatomy. If you have been diagnosed with a uterine anomaly, prioritize a consultation with a reproductive specialist. Focus on your uterus’s function rather than its form.
In fertility, diversity in anatomy does not automatically mean a dysfunction in outcome. Your body is capable of extraordinary things, regardless of the textbook shape of your organs.
Sources: ASRM and ESHRE clinical guidelines on congenital uterine anomalies; Williams Gynecology.
Disclaimer: This report is for informational purposes. If you have been diagnosed with a uterine anomaly, consult with a reproductive endocrinologist. Assessment should be based on your individual history and reproductive goals, not just the visual appearance of your uterus.