For many navigating the path of fertility treatment, the AMH (Anti-Müllerian Hormone) test has become a source of profound emotional weight. A single number can trigger tears of despair or a false sense of security. Yet, in modern reproductive medicine, we are increasingly wary of treating this metric as a “pregnancy possibility score.” AMH is an important clinical indicator, but it is not a prophecy of fate.
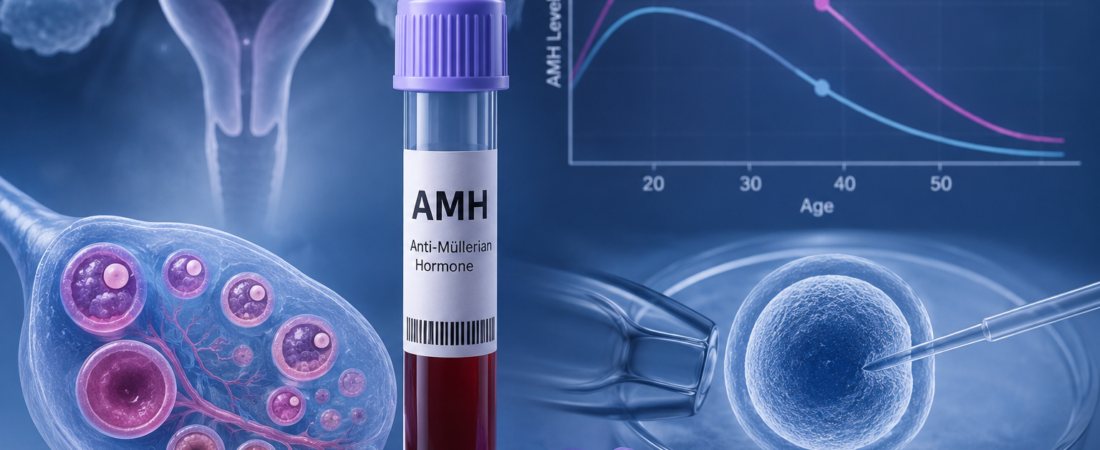
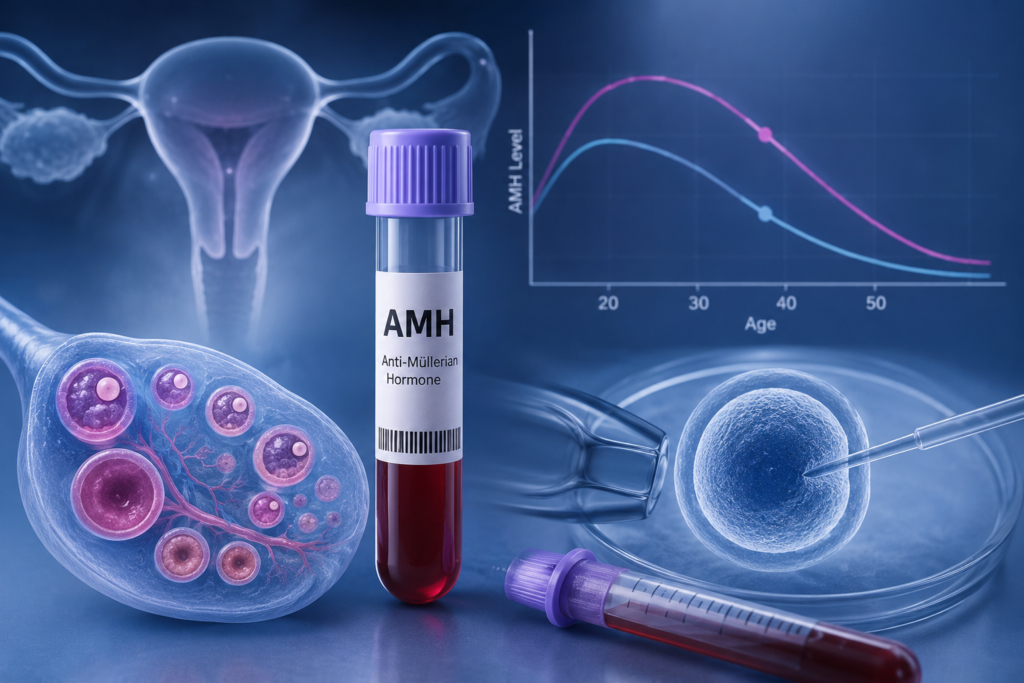
AMH: An Inventory, Not a Quality Audit AMH is produced by the small, developing follicles in your ovaries. Think of it as a gauge of your “inventory”—the quantity of eggs currently available. It is a vital tool for clinicians, but it tells us nothing about the quality of those eggs.
- A low AMH indicates a smaller inventory, but it does not mean the remaining eggs are incapable of resulting in a healthy pregnancy.
- A high AMH suggests a large inventory, but it does not guarantee easier conception or better embryo quality.
The Reality of Clinical Outcomes We frequently see patients with low AMH who achieve natural pregnancies, and patients with high AMH who struggle with recurrent implantation failure. Why? Because reproduction is a “qualitative” game of probability, not a “quantitative” competition. Recent large-scale IVF studies have confirmed that patients with low AMH can—and do—produce embryos with normal chromosomal profiles. The likelihood of a healthy embryo is not zero just because the inventory is limited.
The Age Factor: Time as the Ultimate Variable If AMH is the inventory, age is the clock. Reproductive science emphasizes that chronological age is a more potent predictor of chromosomal integrity (the “quality” of the egg) than AMH. At the end of the day, success in IVF is about finding that one genetically normal embryo. You could retrieve ten eggs that are all chromosomally abnormal, or retrieve only two, one of which results in a healthy pregnancy. The “normal” embryo is a statistical event, not a product of sheer numbers.
The Trap of Fear-Based Marketing The fertility industry often utilizes AMH to create a sense of urgency. Statements like “Your ovarian age is 45” or “You are on the verge of menopause” are often used to pressure patients into immediate, expensive interventions. It is crucial to remember:
- AMH levels can fluctuate based on laboratory methods and cycles.
- AMH is a piece of the puzzle, not the whole picture.
A Holistic Approach to Reproductive Strategy Modern reproductive endocrinologists no longer interpret AMH in isolation. It is now part of a comprehensive assessment that includes:
- Antral Follicle Count (AFC): Visualizing the ovary via ultrasound.
- Hormonal Rhythms: Assessing FSH, LH, and estrogen patterns.
- Systemic Factors: The health of the uterus, partner factors, and metabolic/lifestyle influences.
In IVF, AMH serves a specific clinical purpose: it helps the physician calibrate the stimulation protocol—determining the right dosage of medication to optimize the yield while minimizing the risk of Ovarian Hyperstimulation Syndrome (OHSS). It is a strategic compass, not a diagnostic verdict.
Conclusion: Reclaim Your Agency If you have received a low AMH result, do not view it as a closed door. View it as a signal to be strategic and efficient with your time. If your AMH is high, do not view it as a guarantee; continue to prioritize your overall health and quality.
Fertility is a complex, multi-variable system. AMH is merely one gauge on the dashboard. What matters far more than the number itself is how you and your specialist interpret that data and how calmly you convert it into a concrete, personalized strategy. You are not a number; you are a biological system, and your journey deserves to be defined by strategy, not by fear.
Sources: ASRM Committee Opinion on Ovarian Reserve Testing; EMJ Reproductive Health (2026) on AMH and Embryo Euploidy; clinical consensus on personalized IVF protocols.
Disclaimer: This report is for informational purposes. AMH is a specialized diagnostic marker; please consult with a reproductive endocrinologist to assess your unique reproductive potential and determine the best plan for your specific clinical history.