The word “cyst” on an ultrasound report often triggers an immediate alarm. Patients frequently fear the worst—malignancy—but in clinical practice, the vast majority of ovarian cysts are not cancerous. They are biological events, sometimes mere remnants of the ovary’s cyclical work. The challenge lies in distinguishing the benign “work-in-progress” from the pathological lesions that threaten your fertility.
1. The ‘Work-in-Progress’: Functional Cysts
Every month, the ovary works tirelessly to mature follicles. Sometimes, a follicle doesn’t release properly or leaves a fluid-filled sac behind. These are functional cysts. They are the “remnants of labor.” In most cases, these are transient and resolve on their own. The most common mistake is over-treating these; they are physiological, not pathological.
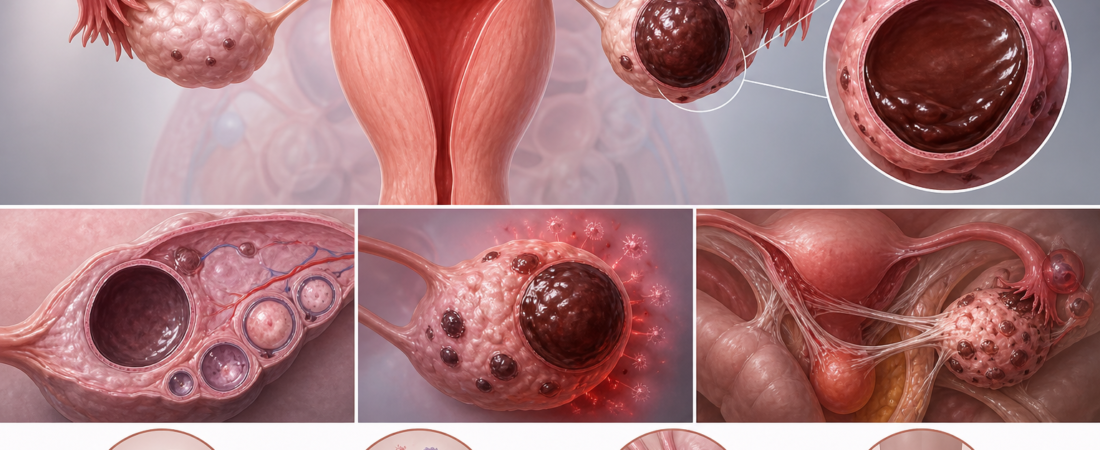
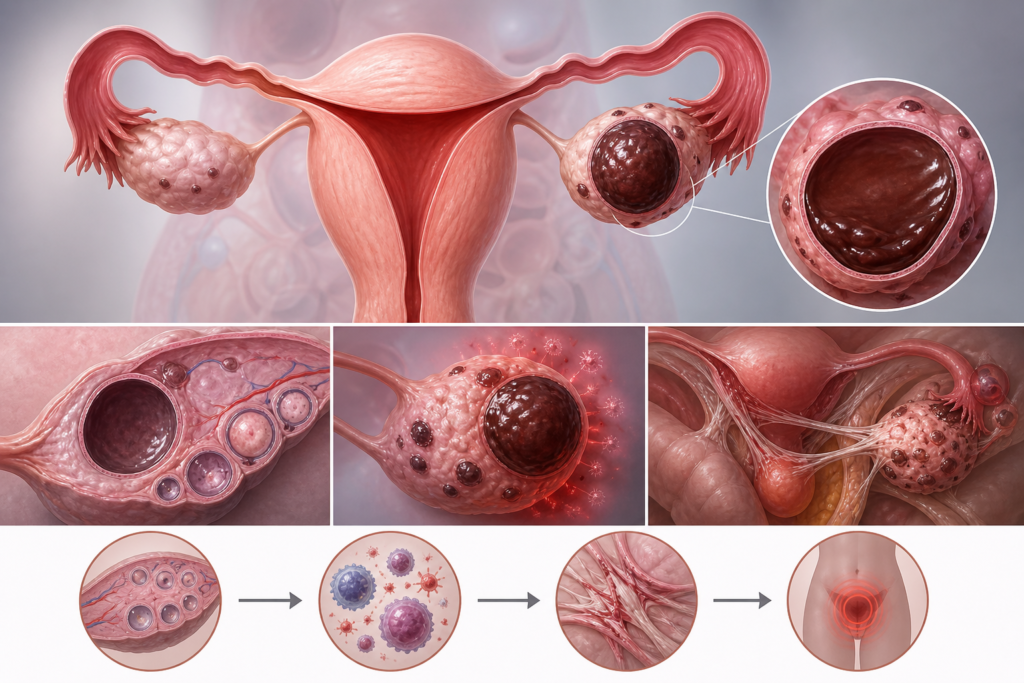
2. The ‘Chocolate Cyst’: Endometrioma
The Endometrioma is fundamentally different. It is an extension of endometriosis—a condition where endometrial tissue thrives outside the uterus. These cysts act as a localized site of chronic inflammation. They don’t just take up space; they disrupt the ovarian environment.
- The Damage: They induce oxidative stress, reduce ovarian blood flow, and limit the space for healthy follicles to grow.
- The Challenge: They often cause adhesions, restricting the movement required for natural conception.
- Management: If you are trying to conceive, the goal is ovarian preservation. While surgery is a traditional route, clinicians now increasingly favor conservative approaches, such as alcohol sclerotherapy, to address the cyst while minimizing collateral damage to healthy ovarian tissue.
3. The Developmental Anomaly: Teratomas (Dermoid Cysts)
Occasionally, a cyst arises not from ovarian function, but from developmental anomalies. These are teratomas, which may contain fatty tissue, hair, or even teeth. Unlike functional cysts, these do not resolve; they are structural. If they grow too large, they risk ovarian torsion (the ovary twisting on itself), which can cause acute pain and loss of ovarian function. These usually require a planned surgical approach.
4. The Silent Sentinel: Ovarian Cancer
The greatest clinical imperative is to distinguish the benign from the malignant. Ovarian cancer is notoriously silent in its early stages. This is why the “eyes” of the clinician are paramount. A specialist uses a combination of ultrasound morphology, size consistency, vascular flow (Doppler), and biomarkers to judge whether a cyst is “ordinary” or requires urgent intervention.
Conclusion: The Necessity of Expertise
When you have a cyst, the most critical question is not just “What is it?” but “What is the strategy?”
- Wait and See: Sometimes, the best treatment is patience. Intervention can sometimes be more harmful than the cyst itself.
- Conservative Intervention: For endometriomas, preserving your egg reserve is the priority.
- Surgical Management: For structural cysts like teratomas, planned removal prevents acute emergencies.
If you are planning for pregnancy, do not settle for a generic diagnosis. Seek a fertility specialist who can differentiate between a passing physiological event and a condition that demands intervention. The goal is to ensure that your ovary remains a functioning factory, not a site of unnecessary damage.
Sources: ESHRE Endometriosis Guideline (2022); Hamdan M et al., “The impact of endometrioma on IVF outcomes: a systematic review and meta-analysis,” Human Reproduction Update (2015).
Disclaimer: This report is for informational purposes. Ovarian findings are highly individual. If you have been diagnosed with an ovarian cyst, consult with a reproductive endocrinologist to determine whether your specific case requires observation, medication, or surgical intervention.