The terms “Adenomyosis” and “Leiomyoma” (commonly known as fibroids) are often lumped together due to their similar names and shared location. However, in a clinical setting, they follow entirely different paths. Failing to distinguish between these two conditions can lead treatment down the wrong path, costing patients their most valuable asset: time.
The Structural Difference: Diffused vs. Localized The fundamental difference lies in their architecture.
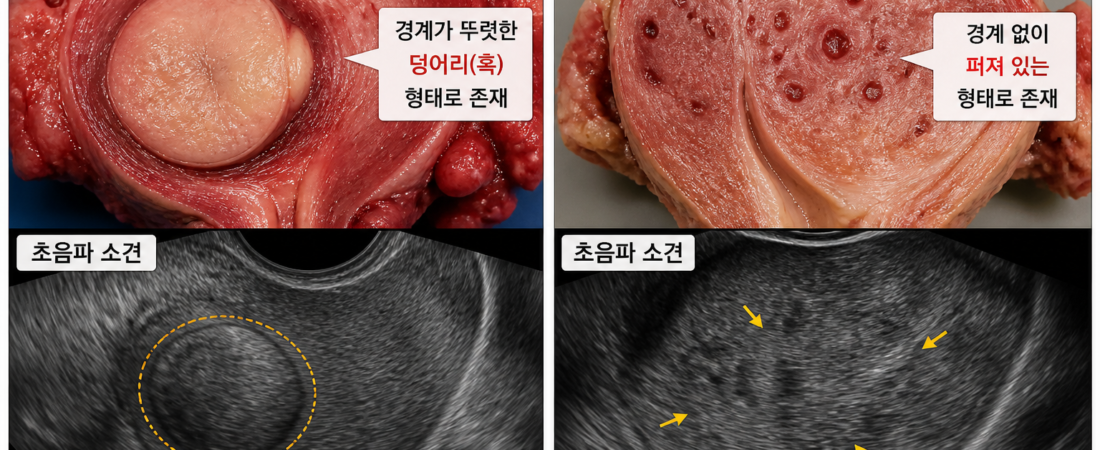
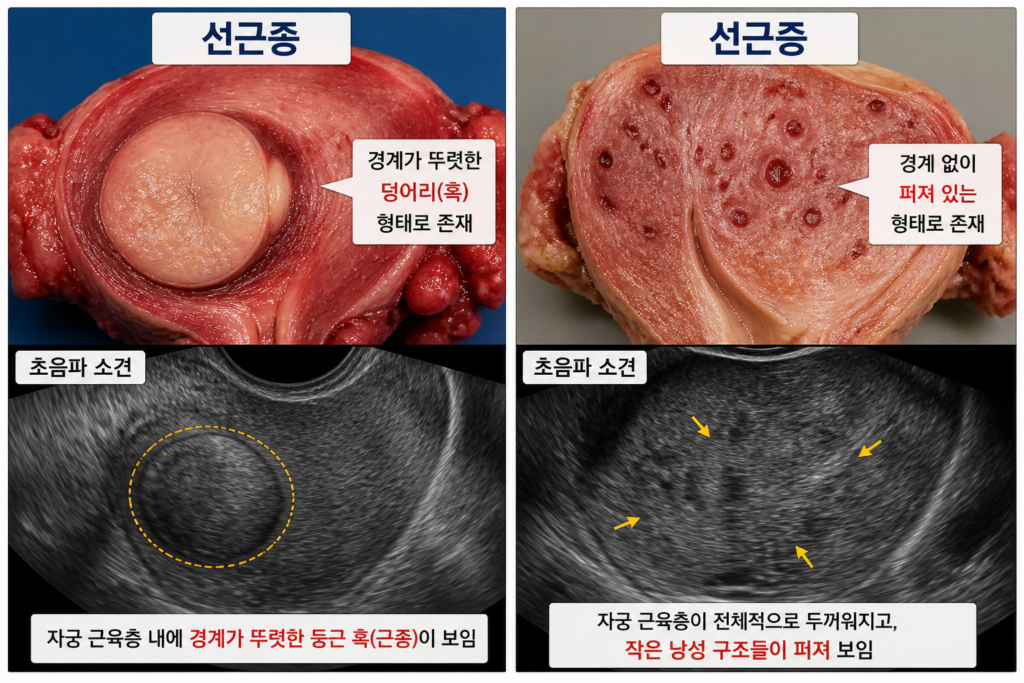
- Adenomyosis: This is a “diffuse” condition. Endometrial tissue infiltrates the muscular wall of the uterus, spreading without clear boundaries and thickening the entire organ. It cannot be “excised” or surgically removed.
- Leiomyoma (Fibroids): These are localized “masses.” They grow as distinct, circumscribed lumps. Their size and location are clear, making them potentially removable if they pose a threat to fertility.
The Impasse: Seed vs. Soil This distinction is not merely academic; it is the deciding factor in fertility outcomes.
- Fibroids: If a fibroid distorts the uterine cavity, its removal often leads to a significant improvement in pregnancy rates.
- Adenomyosis: Because it is diffuse, it cannot be surgically removed. It creates a “poisoned” environment—characterized by chronic inflammation and abnormal muscular contractions—that prevents an embryo from implanting. In this case, the embryo (the seed) might be perfect, but the uterine lining (the soil) is fundamentally hostile.
Treatment Strategy: Different Fights for Different Diseases Because both conditions are fueled by estrogen, ovulation-suppressing treatments can temporarily calm them. However, the intent differs:
- For Fibroids: The goal is often surgical removal. If the fibroid is causing trouble, it is a clear target. If not, it can be monitored. The objective is direct elimination.
- For Adenomyosis: The goal is stabilization. Since we cannot remove the disease, we use hormone suppression to “quiesce” the uterine environment, creating a window of stability for IVF attempts.
The Danger of Misdiagnosis In clinical practice, a single ultrasound is often treated as the final word. Without specialized reproductive expertise, a sonographer might misidentify diffused adenomyosis as mere “uterine enlargement,” or fail to differentiate a complex fibroid.
- The Harm: If adenomyosis is mistaken for a fibroid, a patient might undergo unnecessary surgery that permanently damages the uterine wall. If a fibroid is missed or misidentified, a patient may lose months in unsuccessful IVF cycles when a simple surgical correction could have solved the issue.
Conclusion: Precision Over Generalization In reproductive medicine, time is not just money; it is biological opportunity. The difference between treating a localized mass and a diffused condition is the difference between a successful pregnancy and years of unexplained failure.
If you have been diagnosed with a uterine condition, ask your specialist a simple, vital question: “Is this a distinct mass, or is it a diffused condition spreading through the uterine wall?” Understanding that distinction will change your treatment strategy and, ultimately, the results. When it comes to fertility, precision in diagnosis is the fastest route to success.
Sources: ACOG Practice Bulletins on Leiomyoma and Adenomyosis; ESHRE Guidelines on Endometriosis and Adenomyosis; Williams Gynecology (4th Ed).
Disclaimer: This report is for informational purposes. Uterine diagnosis requires specialized imaging and evaluation. Please discuss your specific anatomical findings with a reproductive endocrinologist.