For those navigating the heartbreak of recurrent implantation failure, the most agonizing phrase is: “The embryo was perfect.” When this happens repeatedly, we must stop questioning the embryo and start examining the stage upon which it must perform. If the uterus—the stage of gestation—is structurally flawed, the outcome is often predetermined, regardless of how high the embryo’s quality might be.
The Spectrum of Uterine Anomalies Uterine anomalies are often described as “rare,” but in clinical practice, they are frequently “rarely diagnosed” issues that silently derail fertility.
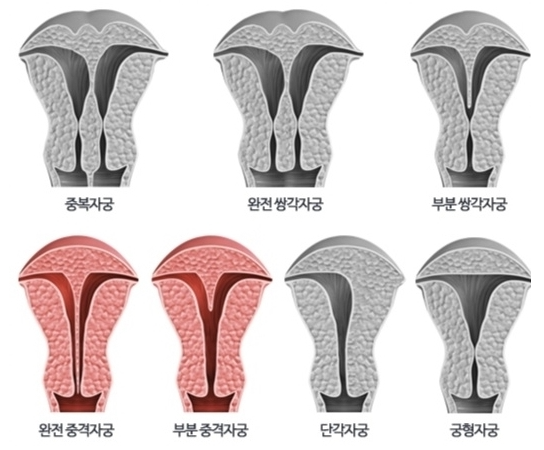
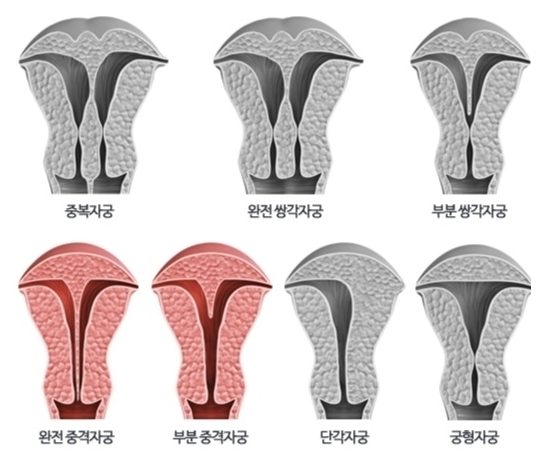
- Septate Uterus (중격자궁): The most common structural anomaly. Externally, the uterus appears normal. Internally, a thin wall—a septum—divides the cavity. Embryos that implant on this fibrous, poorly vascularized wall almost inevitably fail.
- Bicornuate Uterus (쌍각자궁): Here, the uterus is heart-shaped with two distinct horns. While pregnancy can occur, the lack of symmetrical space and structural integrity often leads to fetal malpresentation, preterm labor, or miscarriage.
- Unicornuate Uterus (단각자궁): A half-formed uterus with limited space. It is inherently constrained, making it difficult for a pregnancy to reach full term.
- Didelphic Uterus (이중자궁): A complete duplication of the reproductive tract. While it allows for pregnancy, it carries high risks of preterm delivery and positional complications due to the restricted anatomy of each cavity.
- Arcuate Uterus (궁형자궁): Often dismissed as a “normal variant” because the depression at the top is slight. Yet, this “slight” detail can become a significant barrier for implantation. When it is ambiguous, it is often ignored—to the detriment of the patient.
- T-Shaped Uterus: Characterized by a narrow, distorted cavity. Though historical links to DES exposure are well-documented, similar anatomical distortions are still discovered today, frequently leaving patients without an explanation for why their pregnancies fail to maintain.
- Uterine Hypoplasia (자궁형성부전): A small, underdeveloped uterus. The issue is not just size, but the lack of functional responsiveness—blood flow and hormonal receptivity are fundamentally limited.
Moving Beyond the “Bad Luck” Narrative When these anomalies remain undetected, patients are often told their failures are due to “bad luck.” This is a profound medical oversight. Structural issues cannot be solved by more hormone injections or higher-grade embryos. They require structural interventions—be it surgical correction or specialized IVF protocols designed to work around the anatomical limitations.
The Clinical Call to Action If you have experienced recurrent implantation failure or repeated miscarriages, questioning the anatomy of your uterus is not an option; it is a clinical necessity.
Do not be satisfied with the assumption that your uterus is “normal” based on a cursory ultrasound. Uterine architecture requires a specialized eye—often requiring advanced imaging like 3D ultrasounds, saline sonograms (SIS), or hysteroscopy performed by an experienced reproductive endocrinologist.
Conclusion: Architecture as Destiny In reproductive health, architecture is destiny. You can have the most vibrant seed, but if the soil is shaped like a cliff or a barren rock, nothing will take root. Before you blame the embryo, investigate the space. By ensuring your uterine “stage” is balanced, structurally sound, and receptive, you turn a tilted, precarious path into a viable foundation for life.

Sources: ASRM Practice Committee guidelines on Müllerian anomalies; Williams Gynecology & Novak’s Gynecology (clinical texts on uterine development and pregnancy outcomes).
Disclaimer: This report is for informational purposes. Uterine anomalies are highly individual; a formal diagnosis requires a comprehensive physical exam and specialized imaging by a reproductive specialist.