Even if a highly abnormal sperm cell manages to achieve a fertilization event, the process frequently culminates in an early miscarriage. The definitive biological showdown immediately following fertilization is exclusively governed by paternal DNA integrity.
When men receive their formal semen analysis report, their eyes almost universally lock onto a singular, terrifying metric:
“Normal Morphology: 3%.”
Driven by this raw number, they immediately fall into a state of profound clinical anxiety, reasoning: “If 97% of my sperm is deformed, isn’t my reproductive system severely broken?” To establish immediate clinical reassurance: you do not need to panic. This understanding is only half-taught. In fact, within the real-world parameters of andrology, it is occasionally entirely inaccurate.
Contemporary fertility centers evaluate sperm shapes utilizing the World Health Organization (WHO) reference limits paired with strict morphology criteria (엄격형태기준). Under these rigorous parameters, a normal morphology score of just 4% or higher is officially classified as a completely normal, healthy sample. Evaluating this metric purely through a consumer lens appears bizarre—it dictates that even if 96% of the sample is morphologically abnormal, the patient is still certified as fertile. This completely contradicts everyday intuition. Why does reproductive science operate under such an upside-down standard?
The underlying explanation is remarkably straightforward: the laboratory criteria for morphologically evaluating a human sperm cell are uncompromisingly, brutally strict.
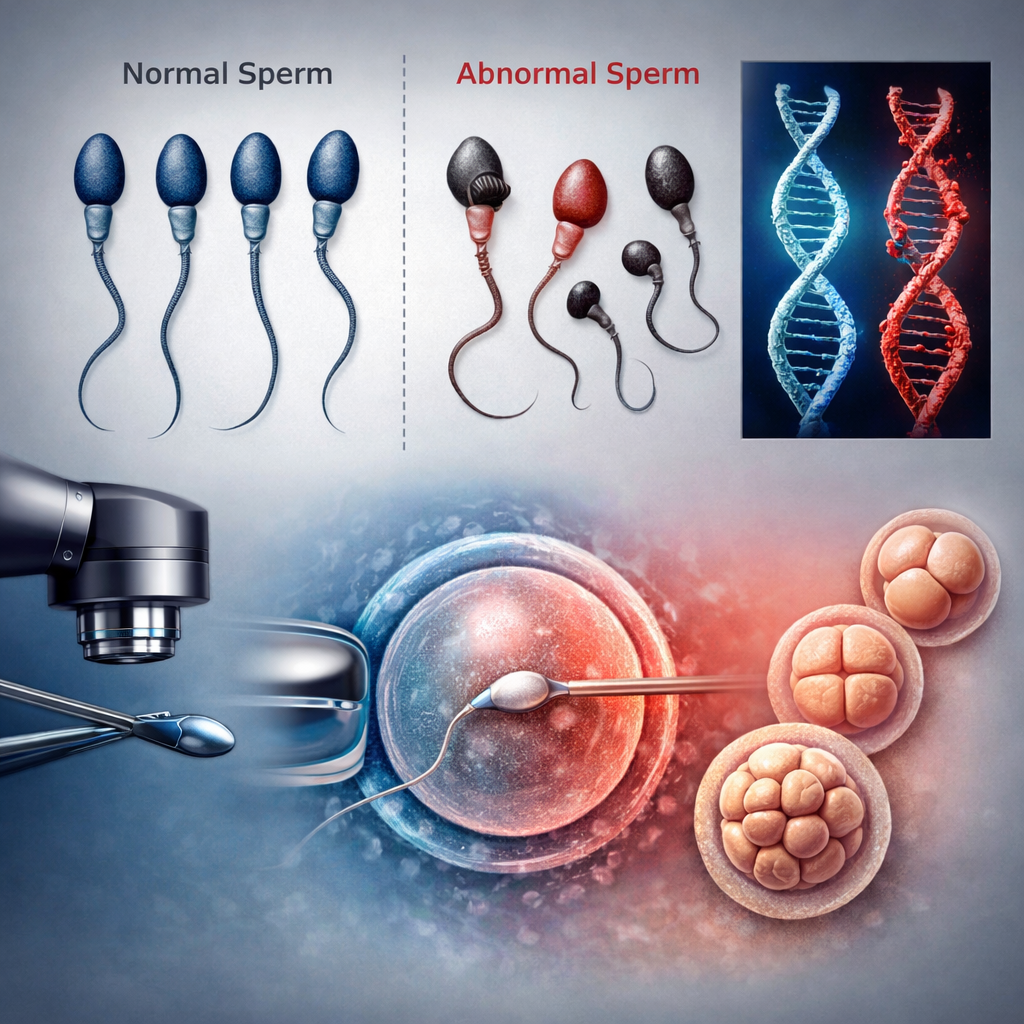
To be certified as “normal,” every single anatomical coordinate must be flawlessly perfect: the head must possess an exact oval dimension with a pristine acrosome proportion, the neck cannot exhibit any erratic angulation, and the tail must maintain a precise length and absolute linearity. If a cell deviates by even a fraction of a micrometer at a single coordinate, it is instantly thrown into the “abnormal” bin.
Consequently, the everyday concept of “usable, functional sperm” and the laboratory definition of an “ideally perfect cell” represent two entirely separate dimensions. The cleanroom cuts lines based on an artificial ideal of structural perfection; the human body does not.
The clinical issue materializes when patients systematically translate this strict numerical data into a flat, flawed formula: “High abnormal morphology equals a guaranteed inability to conceive.”
Real-world natural conception, however, is never structured upon such a simplistic formula.
The female reproductive tract operates as a massive, unyielding biological filtration system. Out of the tens of millions of sperm cells deposited during an encounter, the vast majority are instantly trapped and destroyed at the cervical barrier; those that advance are filtered again through the uterine cavity, leaving only a minute, highly elite handful to successfully reach the fallopian tubes. This arduous transit is, in its own right, a powerful process of natural selection. Cells possessing severe morphological deformities are structurally incapable of navigating this hazardous pathway in the first place.
This is precisely why, in real-world clinical cohorts, couples achieve spontaneous natural pregnancies completely unhindered despite presenting with poor baseline morphology reports. The specific cell that ultimately achieves the milestone of fertilization under these conditions is almost universally a normal or near-normal sperm. Semen is a highly heterogeneous population—a mixed collective of premium, borderline, and deformed cells moving together, where the elite survivors are the ones that dictate the generation of life.
Does this imply that a high concentration of abnormal morphology is entirely devoid of clinical hazard?
The true danger of abnormal morphology manifests long after initial fertilization has concluded, rather than during the act of penetration itself.
Sperm cells presenting with severe structural head defects are statistically and biologically predisposed to harbor elevated levels of paternal DNA fragmentation. In these specific scenarios, the initial fertilization event can comfortably occur. However, as the resulting embryo attempts to navigate its complex downstream cleavage phases, development abruptly freezes, implantation fails, or the pregnancy terminates in a repetitive loop of early clinical miscarriages. This is a profound biological heartbreak repeatedly witnessed within advanced fertility practices.
Consequently, the current overarching trajectory of contemporary reproductive medicine is aggressively shifting away from superficial aesthetics. While morphology remains a valuable baseline indicator, it has surrendered its status as the definitive clinical metric.
Instead, advanced protocols prioritize the absolute integrity of paternal DNA. If a sperm appears visually pristine under a microscope but houses a deeply fractured, damaged genomic sequence, the subsequent embryo is biologically incapable of surviving the developmental timeline. Conversely, if a cell exhibits minor morphological imperfections but retains a highly stable, unfragmented DNA package, it successfully drives full-term healthy live births with remarkable frequency.
As long as a patient’s normal morphology index is maintained at 4% or higher, the statistical probability of achieving a spontaneous natural conception remains completely viable.
The moment the metric slides down into the 2% to 3% corridor, the overall pregnancy rate begins to experience a visible downward skew.
Once the score plunges to 1% or lower, the system crosses the line from normal biological variation into a severe, qualitative deficiency. In scenarios where low morphology is concurrently paired with poor raw count and compromised progressive motility—or when it is documented alongside a history of recurrent miscarriages—the pathology can no longer be evaluated through the lens of simple shape variations.
A sperm cell should never be judged based on how beautifully it competes in a visual lineup; it must be clinically evaluated on its functional capacity to survive the journey, reach the target, execute the molecular connection, and sustain the pregnancy timeline. A report screaming “96% Abnormal Sperm” possesses immense power to induce psychological panic, but true medical empowerment relies entirely on accurately interpreting exactly what that number means.
Crucially, within the framework of modern In Vitro Fertilization (IVF), high abnormal morphology counts lose almost all of their historic clinical weight. Because contemporary cleanrooms deploy advanced Intracytoplasmic Sperm Injection (ICSI, 미세수정) protocols, the embryology team bypasses the requirement for natural transit by manually selecting a single, optimal sperm cell and micro-injecting it straight into the oocyte cytoplasm. Ultimately, the success of the entire cycle is decided not by the aggregate percentage of deformed cells in a cup, but by the pristine genomic quality and functional integrity of that one chosen survivor.
📚 Medical References
- World Health Organization (WHO)
- WHO Laboratory Manual for the Examination and Processing of Human Semen (5th Edition), 2010.
- Significance: The global regulatory manual that established the modern 4% lower reference limit for normal sperm morphology based on strict, standardized parameters.
- Kruger TF, et al.
- “Predictive value of abnormal sperm morphology in in vitro fertilization.”
- Fertility and Sterility, 1986.
- Significance: The pioneering medical literature that formulated the “Kruger Strict Criteria,” proving that highly specialized morphological grading maps out downstream laboratory fertilization kinetics.
- Menkveld R.
- “Clinical significance of the low strict species-specific sperm morphology evaluation.”
- Human Reproduction Update, 2001.
- Significance: A rigorous tracking analysis demonstrating exactly how human sperm shape variations operate as a clinical biomarker for underlying testicular health without fully preventing natural conception.
- Zini A, Sigman M.
- “Are sperm DNA pathogenic parameters clinically useful? A systematic review.”
- Human Reproduction, 2009.
- Significance: Outlines the profound pathogenetic crossover where morphological defects frequently mask underlying paternal DNA fragmentation, directly driving early embryo cleavage arrest.
- Agarwal A, et al.
- “Sperm DNA fragmentation: a new frontier in male infertility evaluation.”
- The World Journal of Men’s Health, 2020.
- Significance: Advanced multi-center study establishing that evaluating genomic integrity provides a vastly superior diagnostic prediction of full-term live birth success compared to traditional visual semen parameters.
Editor’s Note: This content is an analytical commentary prepared by a specialized fertility journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment decisions must exclusively be established through direct consultation with a qualified medical professional.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.