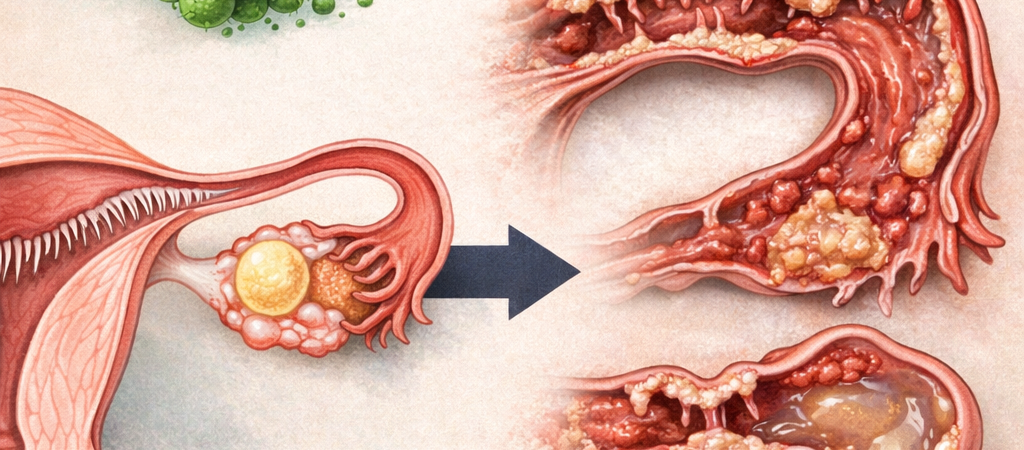
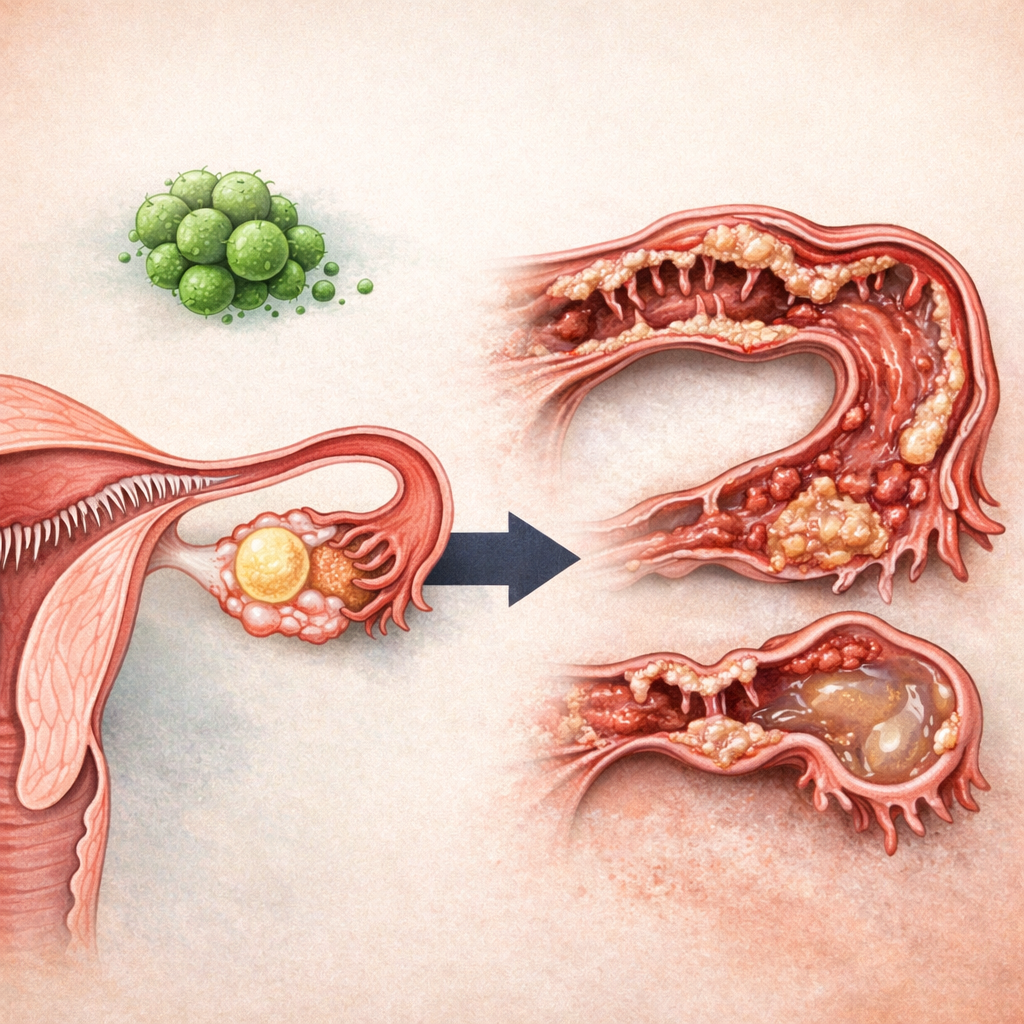
Open but non-functional—a fallopian tube stripped of its biological capability.
The fallopian tubes (난관) are thin, delicate structures measuring approximately 10 to 12 centimeters in length that connect the ovaries to the uterine cavity. They serve as the baseline apparatus designed to capture the ovulated oocyte, provide the precise biochemical arena where fertilization takes place, and comfortably transport the dividing embryo into the womb. Put simply, it is the definitive meeting place for the oocyte and sperm cells. If this pathway undergoes occlusion (막힘) or dynamic pathology, the sperm and egg cannot physically interact, rendering natural conception and Intrauterine Insemination (IUI) virtually impossible.
The foundational clinical misconception is treating the fallopian tube as a passive, hollow pipeline. If it were a mere pipe, clearing a blockage would permanently resolve the issue. In biological reality, however, the fallopian tube is a living, highly coordinated muscular organ. It is a dynamic apparatus that channels synchronized blood flow, maintains waving ciliated cells, and utilizes rhythmic muscular contractions to actively navigate the oocyte toward the uterus. The exact moment we fail to respect this functional reality, we lose our direction when confronted with the repetitive question: “Why did my tube occlude again after a successful surgery?”
Many women navigating infertility express this exact frustration: they underwent a successful tubal cannulation or surgery (나팔관 성형술/개통술), and follow-up imaging confirmed complete patency (개통성), yet the pathway became completely blocked again shortly thereafter. This distressing pattern is not a rare exception; it is a structurally predictable clinical consequence.
The absolute primary driver behind fallopian tube occlusion is chronic localized inflammation. A prominent culprit within this domain is Chlamydia trachomatis—a common sexually transmitted bacterial pathogen. A chlamydial infection does not stop at superficial tissue swelling; it actively drives the systematic destruction of the delicate micro-cilia, causes localized cellular necrosis, and precipitates severe intra-abdominal adhesions (유착).
Parallel etiologies include Pelvic Inflammatory Disease (PID), deep infiltrating endometriosis, and historical pelvic surgeries. The core clinical challenge is that when the acute phase of inflammation clears, it never leaves behind a pristine tissue layer; it leaves a lasting structural scar. Scar tissue lacks the soft, elastic compliance of native fallopian tissue. It is rigid, incapable of coordinated expansion, and once it undergoes narrowing, it is biologically predisposed to collapse back into complete occlusion.
A mechanical tubal cannulation or plastic surgery is simply a localized physical dilation designed to forcibly expand this narrowed segment. It is completely powerless to reverse the structural scarring itself. It is functionally equivalent to forcefully unkinking a badly warped plastic straw; the exact millisecond the external tension is removed, it is a naturally expected progression for the material to revert to its collapsed state over a longitudinal timeline.
Beneath this structural recurrence lies an even more profound biological compromise.
The fallopian tube is never a simple structural tunnel. Its internal mucosal lining is densely populated with microscopic ciliated cells (섬모) that continuously wave in a highly coordinated rhythm to draw the egg inward and gently guide the resulting embryo toward the uterine cavity. Concurrently, the smooth muscle layers execute delicate peristaltic contractions to sustain this directional flow.
The exact moment a fallopian tube endures inflammatory trauma, this fine-tuned machinery undergoes complete failure. The ciliated cells are permanently destroyed, and the muscular motility becomes profoundly blunted. The anatomy enters an ironic state: it is superficially open under high-pressure imaging dye, yet it remains completely deadened and non-functional in real-world application—transforming into an “open but useless관.”
The downstream pathology of this state is remarkably straightforward. In a conduit devoid of physiological flow, fluid stagnation inevitably occurs. Stagnant tubal fluid functions as a biological catalyst for secondary inflammation, which systematically triggers new adhesion cascades, ultimately culminating back in complete physical occlusion. This recurrent blockage following a patent surgery is not an administrative laboratory failure; it is the natural, unyielding path of a permanently compromised tissue system.
Ironical as it may be, the mechanical process of executing the cannulation itself is not entirely harmless. Advancing rigid catheters or inflating therapeutic balloons inflicts acute friction and localized trauma upon the fragile mucosal lining. This micro-endothelial injury can comfortably operate as the exact starting point for a fresh inflammatory healing cascade, meaning the intervention engineered to treat the pathology simultaneously constructs the baseline conditions for its recurrence.
Does this imply that tubal patency surgeries are entirely devoid of clinical utility? Absolute non-utility is inaccurate. For highly specific cohorts presenting with early-stage proximal tubal occlusions (근위부 폐쇄) or transient mucous plugging, mechanical clearing can yield exceptional outcomes.
The danger materializes when this procedure is deployed as a blanket remedy for all forms of tubal blockages. In a fallopian architecture where the ciliated cells have been structurally erased and dense fibrous adhesions have anchored the tissue, a surgery can only briefly force the tunnel open; it possesses zero capability to restore the intricate micro-cellular function required for a child to be conceived.
Ultimately, the diagnostic calculus must abandon the question of “Can we mechanically open this tube?” and prioritize the question of “Does this specific fallopian tube retain functional competence?” Superficial patency is never enough. The capacity for coordinated movement, the structural integrity of the micro-environment, and the ability to safely house a dividing embryo are what truly dictate a live birth. Pregnancy is never a discipline of open pipelines; it is a masterpiece of precise biological function.
At this critical intersection, the reproductive strategy must bifurcate: Do you continue to invest valuable time repeating micro-surgeries to chase a natural conception, or do you pivot to a completely different therapeutic angle?
The overriding variable within this decision matrix is never the superficial success rate of the surgeon’s hands; it is the conservation of the patient’s remaining reproductive timeline. The exact moment a couple exhausts consecutive months waiting on a fundamentally non-functional fallopian tube, their global mathematical probability of conceiving drops drastically as maternal age advances.
A tubal patency surgery is engineered to open a pathway. However, it must never be misconstrued as a treatment capable of transforming a structurally degraded tissue back into a pristine, vibrant organ.
Fortunately, even in scenarios where the fallopian tubes are permanently occluded or functionally deadened, contemporary reproductive science empowers couples to completely bypass this barrier through In Vitro Fertilization (IVF, 시험관아기 시술). IVF completely eliminates the requirement for a functional fallopian architecture by retrieving the eggs directly from the ovaries, fertilizing them within a controlled laboratory cleanroom, and placing the high-potential embryo straight into the uterine cavity. Rather than expending valuable months worrying over a tube that continuously re-occludes, advancing proactively to a highly calculated IVF protocol stands as the far more aggressive and strategically sound path to success.
📚 Medical References
- Practice Committee of the American Society for Reproductive Medicine (ASRM)
- “Role of tubal surgery in the era of assisted reproductive technology: a committee opinion.”
- Fertility and Sterility.
- Significance: The official consensus framework defining the modern clinical limitations of tubal reconstructive surgeries, establishing that IVF yields vastly superior live birth rates in the presence of compromised tubal function or advanced maternal age.
- Practice Committee of the American Society for Reproductive Medicine (ASRM)
- “Salpingectomy for hydrosalpinx prior to in vitro fertilization: a committee opinion.”
- Fertility and Sterility.
- Significance: Outlines the pathogenetic mechanisms where a non-functional, fluid-filled fallopian tube (hydrosalpinx) secretes embryotoxic fluids back into the uterine cavity, detailing why removal or occlusion of the damaged tube is required to safeguard subsequent IVF implantation success.
Editor’s Note: This content is an analytical commentary prepared by a specialized fertility journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment decisions must exclusively be established through direct consultation with a qualified medical professional.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.