The core issue is never the simple presence of a fibroid; it is a profound discipline of clinical judgment and interpretation.
Uterine fibroids (자궁근종) are extraordinarily common, identified in nearly half of all women of reproductive age. Despite this ubiquitous baseline, we are profoundly quick to single out this common entity as the primary “culprit” behind infertility. The underlying reason for this cultural reflex is simple: they are highly visible. They materialize clearly on an ultrasound screen, making them easy for a clinician to explain and remarkably straightforward for a patient to comprehend. Consequently, they are routinely pulled into the absolute center of the diagnostic narrative.
Achieving a pregnancy, however, is never a simple problem of structural anatomy. The uterus is not a lifeless, passive room; it is an intricately coordinated, living tissue responsible for allowing the embryo to attach, invade, and establish vital vascular networks.
Implantation (착상) is far more than a basic process of physical attachment. It represents a highly complex, multi-factorial physiological cascade requiring precise endometrial proliferation, localized immunological modulation, and a radical restructuring of micro-vascular networks. Therefore, the definitive clinical question remains singular: the issue is not whether a fibroid physically exists, but whether this specific lesion is actively fracturing this delicate physiological process.
The non-negotiable variable within this calculus is location.
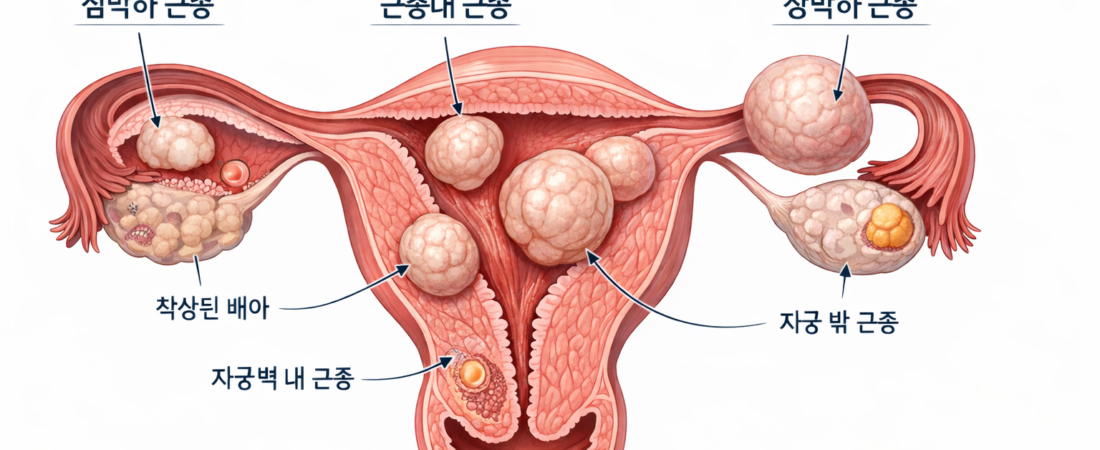
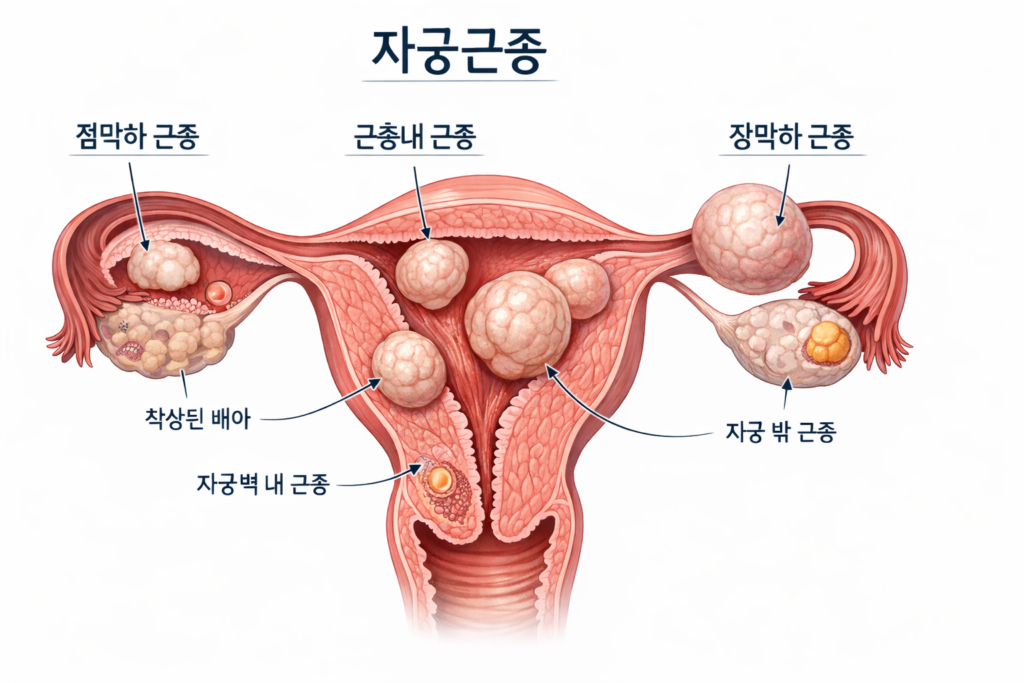
Submucosal fibroids (점막하 근종)—those developing inside the uterine cavity and directly distorting the endometrial architecture—exert a profoundly destructive influence on fertility. They warp the surface topography of the lining, induce chronic localized inflammatory cascades, and severely blunt the molecular receptivity required for attachment. Within this specific anatomical category, a linear reduction in overall pregnancy rates alongside a stark escalation in early miscarriages is consistently documented, rendering active surgical intervention entirely necessary.
Conversely, intramural fibroids (근층내 근종) present a completely different clinical narrative. When these lesions reside strictly within the muscular wall of the uterus without structurally invading the endometrial margin, large-scale data confirms that their negative impact on reproductive outcomes is markedly limited.
Nevertheless, if they present with massive dimensions, exist as multiple multi-focal clusters, or cause subtle sub-clinical distortions of the global uterine cavity, they introduce a distinct probability of altering localized micro-vascular perfusion and disrupting healthy uterine contractility patterns. In short, the answer is neither a universal “everything is completely fine” nor an absolute “this is a guaranteed disaster.” It is a domain that demands deep, tailored interpretation.
Subserosal fibroids (장막하 근종) project outward from the external surface of the uterus, maintaining zero direct anatomical interaction with the internal dynamics of the implantation process. Despite this absolute lack of biological connection, scenarios where surgical intervention is aggressively recommended based strictly on raw size or simple existence remain highly prevalent in active practice. At this precise juncture, the clinical reasoning begins to oversimplify dangerously.
The decision to operate introduces its own volatile set of variables.
While an operative myomectomy (근종절제술) is undeniably therapeutic in meticulously selected profiles, the intervention inherently leaves behind a structural trail of myometrial trauma and permanent scar tissue. This surgical scarring can fundamentally compromise long-term uterine compliance, deaden localized vascular blood flow, and alter the mandatory capacity of the uterus to expand smoothly during a full-term pregnancy.
Crucially, undergoing recurrent uterine operations or enduring extensive surgical incisions can paradoxically degrade the biological environment required to sustain a pregnancy.
Consequently, the current overarching trajectory of contemporary reproductive medicine is absolute: the heavy center of gravity is shifting away from the aggressive eradication of visible lesions, moving toward the systematic preservation of global uterine function.
Ultimately, the intricate relationship linking uterine fibroids to reproductive success cannot be condensed into a single variable. The specific location, raw dimension, and total count of the fibroids are profoundly intertwined with endometrial thickness, real-time vascular perfusion indices, systemic steroid hormone responsiveness, intrinsic embryo quality, and maternal chronological age. The profound diagnostic challenge is that these independent variables continuously exert feedback loops onto one another. If a clinician carelessly touches one variable, the entire system begins to destabilize.
This is precisely why entirely disparate clinical conclusions can be extracted from the exact same ultrasound image depending on the evaluating physician. One practitioner may assert, “We must aggressively excise this fibroid prior to any cycle,” while a parallel specialist counter-argues, “Leave the tissue entirely undisturbed and advance immediately to an active IVF cycle.” Which path is correct?
This radical divergence is never a question of raw textbook knowledge. It is a discipline of deep interpretation, forged ultimately through long-term clinical experience.
A highly seasoned fertility specialist possesses the capacity to look past flat numbers and standardized digital imaging records. They simultaneously evaluate not merely the sonographic location of the lesion, but exactly how much micro-structural distortion it is inflicting upon the endometrium, how historical profiles with identical parameters progressed, and which overarching variable functions as the primary barrier within this specific patient’s unique biological window.
Therefore, the ideal sequence of treatment cannot be dictated by a standardized, rigid formula. Choosing between a pre-treatment intervention followed by an IVF cycle versus executing an immediate IVF harvest followed by targeted management is a sophisticated strategy. This choice must be calculated by synchronizing the patient’s remaining reproductive timeline, chronological age, historical tracking of past cycle failures, and the immediate biological readiness of the uterus simultaneously.
The exact same philosophy governs the surgical scalpel.
While erasing a fibroid appears superficially beneficial, it extracts a steep biological price in the form of tissue scarring and permanently altered vascular dynamics. A master clinician recognizes exactly when not to operate far sooner than deciding when to cut.
In the final analysis, the crossover intersection of uterine fibroids and assisted reproduction lacks a single, absolute template answer. An identical fibroid can stand as a critical target for immediate surgical removal in one patient, while functioning as an entity that must be left completely unviolated in another. The definitive element that constructs this profound difference is never the raw laboratory report; it is the analytical power of the mind interpreting the data.
Therefore, the final diagnostic focus must be reframed. The question is no longer whether this fibroid is inherently problematic, but rather: Is the clinical team accurately reading the entire global situation? When a definitive treatment choice is built upon a foundation of deep, experience-driven interpretation, that chosen path is already comfortably standing halfway toward a successful outcome.
📚 Medical References
- Practice Committee of the American Society for Reproductive Medicine (ASRM)
- “Evaluation and treatment of uterine fibroids: a committee opinion.”
- Fertility and Sterility.
- Significance: The official consensus framework detailing the precise diagnostic guidelines and management metrics for evaluating fibroids within an active infertility workout.
- Pritts EA, Parker WH, Olive DL.
- “Fibroids and infertility: an updated systematic review of the evidence.”
- Fertility and Sterility.
- Significance: A landmark systematic review establishing the definitive statistical correlations linking specific anatomical fibroid locations (submucosal vs. intramural vs. subserosal) to baseline implantation and live birth rates.
- Somigliana E, et al.
- “Uterine fibroids and reproductive outcomes: a comprehensive review of the clinical data.”
- Human Reproduction Update.
- Significance: Longitudinal analyses detailing the systemic impact of intramural lesions on local endometrial perfusion and global myometrial contractility patterns.
- Stewart EA.
- “Uterine fibroids.”
- The Lancet.
- Significance: A comprehensive clinical overview mapping out the underlying pathophysiology, global epidemiology, and tissue-level characteristics of uterine leiomyomas across the lifespan.
- Donnez J, Dolmans MM.
- “Uterine fibromatosis: moving toward custom-tailored medical and surgical management.”
- New England Journal of Medicine.
- Significance: Advanced surgical literature detailing the non-negotiable requirement for customized, function-preserving strategies over standard radical lesion removal in childbearing cohorts.
Editor’s Note: This content is an analytical commentary prepared by a specialized fertility journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment decisions must exclusively be established through direct consultation with a qualified medical professional.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.