

Does the mere presence of a regular menstrual cycle guarantee the absolute capacity to conceive? The definitive clinical answer is no.
Within the framework of advanced In Vitro Fertilization (IVF), tracking the raw number of retrieved oocytes is no longer the definitive diagnostic focus. The core clinical challenge resides entirely within a singular question: Can even one solitary, genetically normal oocyte survive that numerical harvest?
A woman’s lifelong ovarian reserve is permanently fixed during embryonic development and undergoes a continuous, irreversible depletion across her lifespan. Initiating at an estimated 6 to 7 million oocytes during the fetal stage, the pool drops to roughly 1 to 2 million at birth, and declines further to approximately 300,000 to 500,000 cells by the onset of puberty.
By the chronological age of 30, the count is reduced to approximately 100,000; by age 40, it plunges below 10,000; and by age 45, the remaining reserve drops precipitously to fewer than 1,000 oocytes. While evaluating these raw metrics on paper might suggest that a baseline supply still exists, a far more critical biological collapse operates simultaneously: oocyte quality degrades exponentially faster than the decline in raw quantity.
What occurs within the reproductive system at the age of 45? Even if residual oocytes physically reside within the ovarian cortex, the presence of functionally viable cells approaches near-zero parameters. The baseline incidence of numerical chromosomal abnormalities (aneuploidy) scales drastically to 70–90% or higher, and the statistical probability of yielding a genetically normal euploid embryo collapses. Consequently, the rate of spontaneous natural conception drops to a mere 1–2% annually. At this stage, the primary barrier is not a complete absence of eggs, but an absolute scarcity of usable, competent eggs.
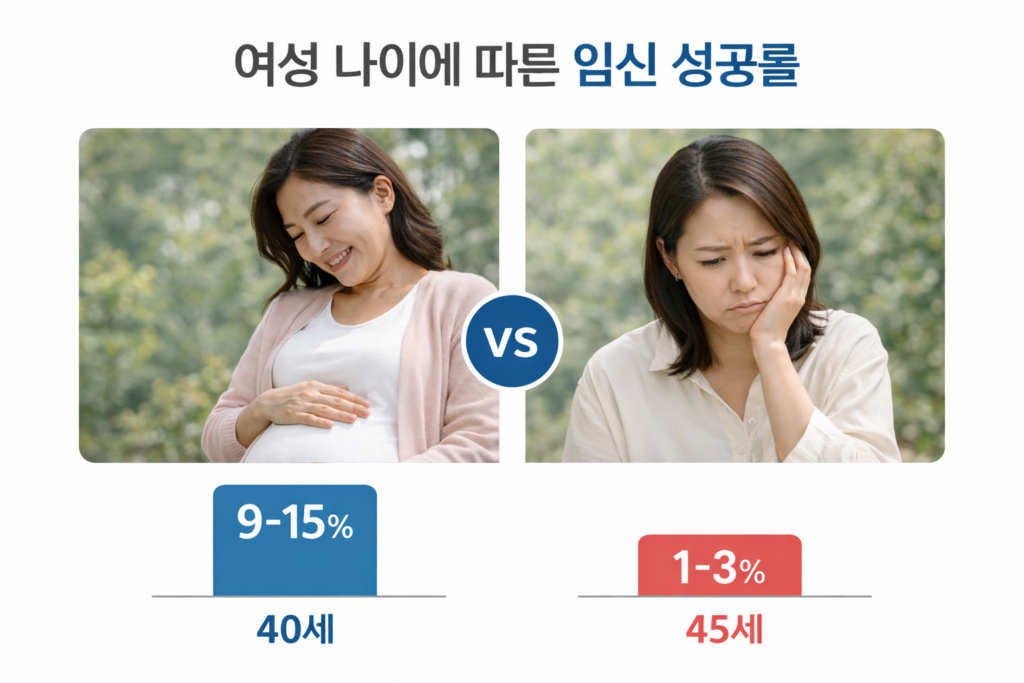
It is precisely this biological divergence that draws a definitive boundary line between the age of 40 and 45.
Up to the chronological age of 40, a calculated clinical strategy remains mathematically viable. Although the baseline probability of securing a genetically sound oocyte has already declined below the 50% threshold, the underlying reproductive architecture still functions. A clinical framework establishing that harvesting a cohort of 10 oocytes can potentially yield one viable embryo remains statistically valid. In active clinical practice, securing a larger pool—ranging precisely between 8 and 15 retrieved oocytes—is required to reliably drive a positive reproductive outcome.
Under these parameters, failed cycles will undeniably occur. However, within this specific age corridor, repeating the stimulation protocol remains entirely rational because the baseline biological probability remains actively operational.
The defining crisis materializes at the age of 45, where that statistical probability effectively shuts down. Securing an identical harvest of 10 oocytes no longer carries the same biological value. The probability of encountering a normal euploid egg drops below 5%, residing realistically between a volatile 1% and 3% margin. While it appears logical to simply scale up the raw numbers to offset this deficit, the foundational calculus of stimulation completely breaks down at this threshold; assuming a harvest of 20 or 30 oocytes is a metric that real-world ovarian biology can no longer fulfill.
Oocytes captured with immense clinical effort at this advanced age exhibit an exceptionally high rate of developmental arrest before completing in vitro culture. A patient can endure multiple consecutive IVF cycles, yet the process frequently concludes with zero transferable blastocysts.
Therefore, for individuals who intensely desire to achieve a pregnancy and maximize their reproductive window, initiating active intervention—whether attempting spontaneous natural conception or advancing directly to In Vitro Fertilization (IVF)—must be aggressively pursued prior to the absolute biological ceiling of 43 years of age. Once a patient surpasses the threshold of 44, the probability of successful conception drops to a near-zero baseline, and capturing viable oocytes becomes profoundly difficult.
At the age of 40, attempting a pregnancy operates as a strict game of statistical probability; the odds have markedly declined, but the system is still functional.
At the age of 45, it becomes an entirely different paradigm. It ceases to be a question of adjusting probabilities and becomes a fundamental breakdown of biological architecture. While patients ask the exact same questions, the human reproductive system delivers a completely different answer.
The absolute moment a woman crosses the chronological threshold of 45, the clinical narrative completely abandons the metric of “how many oocytes were captured,” centering entirely on whether a single, genetically sound egg can survive the biological timeline. Achieving that outcome is extraordinarily difficult. Consequently, navigating a pregnancy attempt after the age of 45 means the timeline required to capture that one solitary, healthy oocyte can stretch indefinitely.
📚 Medical References
- Wallace WHB, Kelsey TW.
- “Human ovarian reserve from conception to the menopause.”
- Human Reproduction Update.
- Significance: The definitive mathematical model tracking the precise, lifelong chronological depletion of the human oocyte pool from the fetal stage through menopause.
- Franasiak JM, Forman EJ, Hong KH, et al.
- “The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies.”
- Fertility and Sterility.
- Significance: A massive multi-center clinical data analysis establishing the linear, unyielding escalation of embryo chromosomal abnormalities as maternal age advances toward the mid-40s.
- Hassold T, Hunt P.
- “To err (meiotically) is human: the genesis of human aneuploidy.”
- Nature Reviews Genetics.
- Significance: Outlines the precise molecular and cellular mechanisms governing maternal meiotic spindle degradation, explaining why older oocytes experience a near-total failure in proper chromosomal segregation.
Editor’s Note: This content is an analytical commentary prepared by a specialized fertility journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment decisions must exclusively be established through direct consultation with a qualified medical professional.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.