
There is a phrase that patients undergoing In Vitro Fertilization (IVF) repeat with the highest frequency:
“Please select the best oocytes to proceed with fertilization.”
This request, however, is fundamentally flawed from the very beginning. An oocyte is not a commodity that can be superficially selected.
Furthermore, there is a more critical truth: oocytes that appear visually flawless on the surface are not nearly as viable in reality as one might expect.
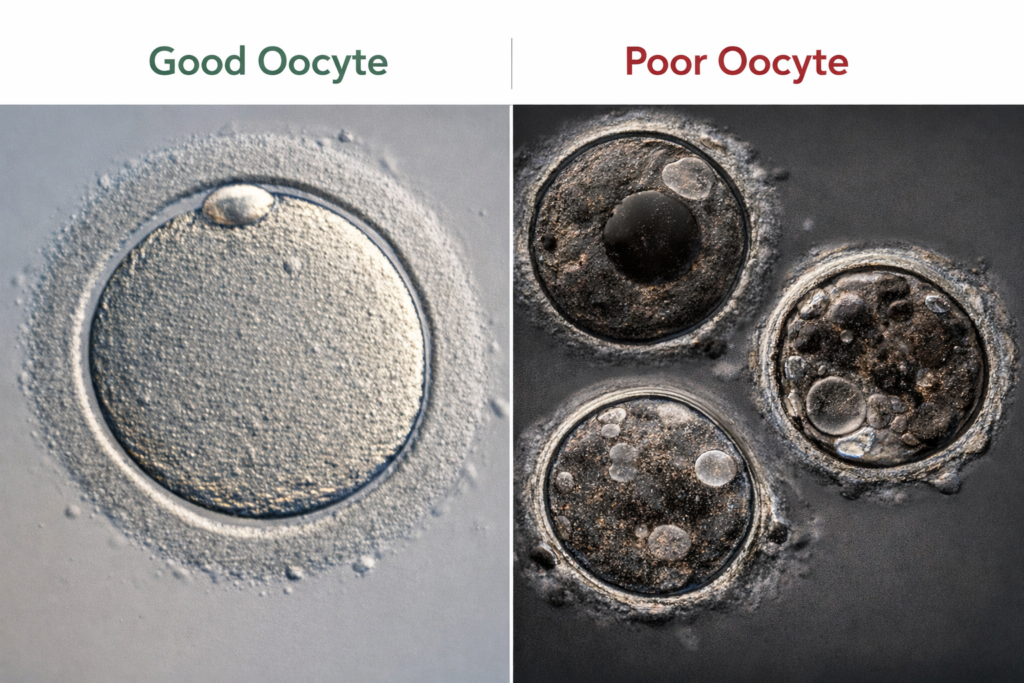
Under a standard laboratory microscope, most oocytes appear remarkably similar. They are generally spherical, adequate in size, and relatively clear. Because of this uniform appearance, an inexperienced embryologist can easily become confused; every cell looks viable.
Conversely, a seasoned embryologist will systematically exclude several oocytes right from the start. The underlying reason is straightforward: they evaluate the internal architecture rather than the external façade.
The primary variable under evaluation is maturity. The laboratory strictly utilizes oocytes at the MII (Metaphase II) stage, which possess a visible first polar body. This baseline step is common practice.
The real clinical challenge initiates immediately after this point. Even among oocytes classified at the exact same MII stage, reproductive outcomes diverge entirely. This is the precise intersection where true selection begins.
The embryologist meticulously evaluates the cytoplasm. This is an area where textbook guidelines fail to capture the active clinical landscape.
In real-world practice, the assessment relies on deeply intuitive tactile and visual markers. Terms such as “cloudy,” “coarse,” “aggregated,” or “subtly iridescent” are far more descriptive of the reality. A master embryologist reads these microscopic nuances instantly. While severely compromised oocytes are comfortably excluded early on, the primary hazard lies in the borderline oocytes.
Borderline oocytes appear entirely normal on the surface. They possess a clear polar body and exhibit standard dimensions. Consequently, they are routinely selected for the cycle.
Yet, it is precisely these oocytes that exhibit the highest failure rates during embryonic development. This is because their internal metabolic integrity and cytoplasmic machinery are already experiencing sub-clinical instability.
Oocytes displaying intracellular vacuoles operate under a similar clinical dynamic. Vacuoles appear as minute, air-bubble-like structures within the cell. While they might be misinterpreted as a minor morphological variation, clinical data directly links them to underlying cytoplasmic abnormalities.
Fertilization itself remains entirely achievable. However, subsequent cellular cleavage pathways consistently report an increased incidence of blastomere asymmetry and developmental disruption.
There is another vital fact that patients must understand: oocytes do not yield reproductive success in a sequential order dictated by their visual grade. The most aesthetically perfect oocyte can undergo sudden developmental arrest, while a cell that showed minimal promise can sustain development to full term. Consequently, relying strictly on visual selection has clear biological limits.
Ultimately, the cornerstone of successful embryology is not “what to select,” but “what to exclude.” A senior embryologist prioritizes exclusion over selection. This rigorous baseline criterion is forged through longitudinal clinical outcomes rather than rigid theoretical manuals.
The process does not conclude with selection. An oocyte is profoundly influenced by the microscopic manipulations that follow the selection phase.
During an Intracytoplasmic Sperm Injection (ICSI) protocol, variables such as the precise site of needle entry, injection velocity, and cytoplasmic stabilization can drive the exact same oocyte toward entirely disparate outcomes. Simply put, even if a premium oocyte is selected, it will fail if it undergoes mechanical micro-trauma during injection; conversely, a borderline oocyte can yield a viable embryo if it is handled with absolute stability.
The core question must be reframed. Instead of demanding, “Please select the best oocytes,” patients should ask: “Does the laboratory possess the expertise to handle this specific oocyte flawlessly?”
An oocyte cannot be deceived by superficial shapes. Human operators, however, are highly prone to being deceived.
Ultimately, oocyte selection is never a challenge of simple visual aesthetics. It is a discipline of deep experience inextricably linked to clinical outcomes. Only an embryologist who has accumulated vast patterns of which oocytes sustain development and which cells arrest mid-cycle can make an accurate clinical judgment.
This conclusion is remarkably simple, yet uncompromisingly cold: a healthy oocyte is not something you casually select. It is something recognized only by a professional who has successfully driven outcomes to fulfillment.
📚 Medical References
- Rienzi L, Vajta G, Ubaldi F.
- “Predictive value of oocyte morphology in human IVF: a systematic review.”
- Human Reproduction Update. 2011;17(1):34–45.
- Significance: Establishes that visible cytoplasmic variations and structural alterations within the oocyte are key indicators of underlying quality, directly impacting downstream embryonic development.
- Alpha Scientists in Reproductive Medicine, ESHRE.
- “Istanbul consensus workshop on embryo assessment.”
- Human Reproduction. 2011;26(6):1270–1283.
- Significance: The international consensus guidelines that define standard grading metrics for oocytes and embryos, providing the clinical criteria for identifying morphological abnormalities like vacuoles.
Editor’s Note: This content is an analytical commentary prepared by a specialized medical journalist through the collection and evaluation of domestic and international reproductive medicine research, clinical policies, and statistical data. All medical diagnoses and treatment plans must exclusively be established through direct consultation with a qualified fertility specialist.
Image Source: AI-generated (ChatGPT, OpenAI) / Provided solely as a supplemental visual aid for conceptual understanding.